In collaboration with the Fairfax County and Loudoun County Health Departments, the Virginia Department of Health (VDH) is investigating a confirmed case of dengue virus infection in a resident who did not have known travel outside of Virginia prior to illness onset. This is the first documented case of locally acquired dengue in Virginia. The patient is known to have been in close proximity to a recent internationally acquired case in a Virginian who was diagnosed a couple weeks prior. Dengue viruses are spread to people through the bites of infected Aedes species mosquitoes. Transmission of the virus likely occurred when a local mosquito bit the internationally acquired case while infectious and subsequently infected the second case. There is no evidence of continued transmission and no additional reports of locally acquired dengue cases at this time. The potential risk for acquiringdengue virus in Virginia remains low.
VDH is working with local partners to monitor for any additional dengue cases and conduct surveillance of mosquitoes that can carry dengue viruses.
Given this recent report of local transmission, providers should:
Advise patients on strategies to prevent mosquito bites. This will not only reduce risk of dengue but also of mosquito-borne disease endemic to Virginia, such as West Nile Virus.
Aedes mosquitoes, which can transmit dengue virus, breed in water-filled containers that may be as small as a bottle cap. Advise patients to “tip and toss” containers around their homes and businesses that may hold water.
Obtain a travel history for all patients presenting with acute febrile illness.
Consider dengue in patients presenting with fever who live in or recently traveled to areas with risk of dengue.
Consider dengue in patients without travel history if presenting with an acute febrile illness and strongly suggestive symptoms, including eye pain, muscle pain, joint pain, and bone pain.
Alert your local health department immediately if you suspect dengue illness in a patient who has no history of travel to areas with risk of dengue or other risk factors for dengue infection, such as receiving a blood or organ transplant.
Obtain diagnostic testing in suspect cases of dengue virus infection.
Review the Centers for Disease Control and Prevention (CDC) guidance on dengue case management, including recommendations by patient groups.
Dengue Overview
Most dengue cases reported in the United States are related to international travel to areas with known risk of dengue. As the types of mosquitoes that can spread dengue viruses are common in many areas of the United States, limited, local transmission of dengue has been documented in the United States. Rarely, dengue is spread in laboratory or healthcare setting exposures through blood transfusions, organ transplants, or needlestick injuries.
Dengue can range from asymptomatic infection or mild illness to severe disease. The typical incubation period is 5–7 days. The usual clinical presentation includes acute onset of fever accompanied by any of the following symptoms: severe headache, retro-orbital pain, myalgia, nausea and vomiting, arthralgia, and macular or maculopapular rash. Mild symptoms of dengue can be confused with other illnesses that cause fever. Symptoms of dengue typically last 2–7 days. Most people will recover after about a week.
Approximately one in 20 infected people develop severe dengue, which is a medical emergency. Symptoms of dengue can become severe within a few hours. Severe dengue can result in shock, internal bleeding, and death. Warning signs that have been associated with an increased risk for progression to severe dengue include:
Severe abdominal pain or tenderness
Persistent vomiting (≥3 episodes in 1 hr. or ≥4 episodes in 6 hrs.)
Clinical fluid accumulation (e.g., pleural effusion, ascites, or pericardial effusion)
Mucosal bleeding
Altered mental status
Liver enlargement
Progressive increase of the hematocrit (in at least 2 consecutive measurements taken 6 hours apart).
Laboratory Testing
Diagnostic test recommendations for dengue depend on the patient’s phase of illness. In the acute phase (0-7 days after symptom onset), diagnostic testing should include both a nucleic acid amplification test (NAAT), such as RT-PCR, and an IgM antibody test. Dengue virus antigen testing for nonstructural protein 1 (NS1 antigen test) can also be used to confirm infection. In the convalescent phase (>7 days post-symptom onset), only IgM antibody testing is recommended. If the timing of symptom onset is not clear, both NAAT and IgM should be ordered.
If you have additional questions about dengue, please contact [email protected].
On behalf of the entire VDH team, thank you for your partnership, dedication and determination in keeping Virginians safe and healthy.
https://www.msv.org/wp-content/uploads/2021/11/msv-logo_340x156.png00varmshttps://www.msv.org/wp-content/uploads/2021/11/msv-logo_340x156.pngvarms2026-08-04 18:00:262026-08-04 18:00:27VDH Identifies a Locally Acquired Case of Dengue Virus Infection in a Northern Virginia Resident
The Commission shall provide public access to information regarding the Virginia fee schedules for medical services, by categories of providers of fee scheduled medical services and for each medical community, through the Commission’s website.
2026 Schedule Updates
Medical Inflation Adjustment: Maximum fees for codes carried over from the 2024 MFS to the 2026 MFS increased by 3.4% to reflect two years of medical inflation.
Addition of New Codes: DRG, CPT, and HCPCS codes introduced in 2024 and 2025 were added to the 2026 MFS when they replaced terminated codes from the 2024 MFS, based on crosswalks provided by the American Medical Association.
Removal of Retired Codes: Codes retired prior to January 1, 2025, were excluded from the 2026 MFS.
Fee Adjustments for Revised Definitions: Codes with revised definitions in 2024 or 2025 had their maximum fees updated accordingly.
The approved 2026 MFS and a detailed listing of all changes effective January 1, 2026, are available on the Commission’s website, accessed here.
MFS Administrative Determination Notice
Medical Fee Services announced an update to the Administrative Determination Notice in a redesigned format.
Key revisions include:
Line‑Level Adjustment Details
Each claim line now explicitly identifies the Ground Rule adjustment(s) applied.
Fee Calculations
Maximum fees are displayed as the calculated amount per code, ensuring transparency in fee determination.
MFS Administrative Determination Notice Tutorial
Training on the use and interpretation of the new Administrative Determination Notice and is available below, or on VWC’s YouTube channel.
Frequently Asked Questions
Q: I am a tertiary hospital located outside of the state. Is it possible to use the calculator to determine Type One Teaching Hospital fees for my facility? If yes, where is that information entered?
A: Type One Teaching Hospitals are state of Virginia‑owned teaching hospitals that have been designated as such since January 1, 1996. These facilities exist only in Regions 2 and 3 and have maximum fee values assigned to all applicable billing codes. As a result, if your service region is outside Regions 2 or 3, or if the billing code does not qualify, selecting a Type One Teaching Hospital will return a result of Not Applicable (N/A).
Q: The payment received is not what is listed in the VA Medical Fee Schedule. What falls under the jurisdiction of the VA Medical Fee Schedule?
A: Payments from payers may be lower or higher than the medical fee schedules. In the absence of a contract, the Virginia Medical Fee Schedule is a tool that the Commission uses to determine the fee schedule maximum assigned amount for medical claims that have an award on file and a dispute has been submitted to the Commission to determine reimbursement for medical treatment provided to an injured worker.
Q. There is an award for medical benefits; however, the payer denied payment for medical services rendered to the injured worker and I do not think this is correct. Is there anything the Virginia Workers Compensation Commission can do?
A: In the event the medical provider and payer cannot agree on proper reimbursement for medical services rendered under the Virginia Workers Compensation Act, a request may be submitted to have the dispute reviewed administratively. An MFS Dispute Request form can be filed directly with the Commission. More information on the MFS dispute Resolution process can be locatedhere.
Q: I’ve submitted my bill to the payer for reimbursement, I don’t agree with what they are recommending for payment, the explanation of review indicates I should forward a request for reconsideration to the Commission.
A: The Commission determines the award status for medical benefits, establishes medical fee schedule reimbursement rates for medical treatment provided, and issues determinations for disputes that are submitted to the Commission for reimbursement disagreements. The Commission does not review reconsideration requests or issue payments for medical treatment provided to injured workers. Requests for reconsideration must be filed directly with the payer.
Q: A code was denied as not being listed in the fee schedule, does this mean that payers do not have to pay for these medical services?
A: No, this does not mean that payers do not have to issue a payment. The Ground Rules document identifies that the absence of any code from the medical fee schedule does not mean that the medical services corresponding to that code are services outside of the scope of the coverage provided by the Virginia Workers’ Compensation Act. If the parties cannot reach an amicable agreement for the reimbursement amount for the code. Either party may submit a dispute request to the Commission to have the fee schedule maximum assigned amount determined.
Q. We are establishing our business rules for reimbursement using the medical fee schedule maximum assigned amounts. If there is not a maximum amount listed in the schedule we cannot come to an agreement with the medical provider for reimbursement, can we just pay 80% if billed charges?
A. The Medical Fee Services Department cannot provide directions on any stakeholder’s internal business processes. The Medical Fee Services Department can review the issues identified in a dispute submitted to the Commission and will issue a formal determination that defines the fee scheduled maximum assigned amount.
Q. The medical bill includes implant charges that are excessive, why does the Medical Fee Services Department not review the charges to determine the usual and customary amounts?
A. The implementation of the Virginia Medical Fee Schedules effective on 01/01/2018, replaced the usual and customary standard for implant charges for all dates of service on or after the effective date. Under the Virginia Workers’ Compensation Medical Fee Schedules, reimbursement rules for implantable medical devices depend entirely on how the device is coded and how the maximum fee is calculated.
Q. Medicare National Correct Coding Initiative (NCCI) edits include specific code combination edits that limit incorrect code combinations. Why was a code I denied allowed in the Medical Fee Service’s administrative determination?
A. There are often ambiguous details within complex medical procedures that are often not captured in simply reviewing the numerical code. The Medical Fee Services Department reviews the medical services first and then determines if the code used to describe the services meets applicable coding conventions.
Q. We are in another state; however, our facility has a Level I trauma center designation, are we eligible for the traumatic injury exclusion?
A. No, The Ground Rules document definition for Level I or Level II Trauma Center ” means a hospital in the Commonwealth designated by the Board of Health as a Level I or Level II trauma center pursuant to the Statewide Emergency Medical Services Plan developed in accordance with § 32.1-111.3
2026 MFS Symposium
October 20, 2026
Save the date for the 2026 MFS Symposium, again held during the first day of the Virginia Workers’ Compensation Commission’s Educational Conference on October 20, 2026. Join the MFS Department to gain additional insights into the following topics:
Navigating the MFS Dispute Resolution Process
Navigate the dispute submission process.
Review documentation requirements including required billing forms and supporting information.
Gain understanding of impact of extension requests and how they affect timelines.
Understanding the MFS Administrative Determination
How determinations are generated and how to interpret payment adjustments or denials.
Brief overview of the MFS Calculator, required inputs, and alignment with current ground rules.
What to know about calculator limitations and when manual review applies.
Post‑MFS 2026 Issue Submission
Snapshot of the biennial revision submission process and stakeholder roles.
Common stakeholder questions identifying specific unlisted codes
How missing codes are identified, validated, and incorporated.
Overview of DRG versioning for the 2026 release and its impact.
What’s Next for MFS
Preview of upcoming enhancements, including updated forms and expanded MFS WebFile functionality.
Planned improvements to the calculator interface and logic transparency.
On July 14, 2026, the Centers for Medicare & Medicaid Services (CMS) released the Calendar Year (CY) 2027 Revisions to Payment Policies under the Medicare Physician Payment Schedule (PFS) and Other Changes to Part B Payment and Coverage Policies proposed rule and fact sheet. The proposed rule includes proposals related to Medicare physician payment and the Quality Payment Program (QPP). If finalized, these policies will take effect on January 1, 2027, unless otherwise noted. The American Medical Association (AMA) will submit detailed comments by the September 14, 2026 deadline and encourages Federation members to do the same. The AMA will provide a draft version of its comments to Federation members in advance of the deadline.
I. PAYMENT PROVISIONS
CY 2027 Medicare Conversion Factors
For the second year, there are four proposed conversion factors, as outlined below:
Medicare Conversion Factor
Medicare Anesthesia Conversion Factor
For APM QPs
For non-APM QPs
For APM QPs
For non-APM QPs
$33.1693 (-1.19%)
$32.8409 (-1.68%)
$20.4165 (-0.89%)
$20.2143 (-1.38%)
These conversion factors reflect:
Expiration of the temporary 2.5 percent update for CY 2026 included in H.R.1
A 0.53 percent budget neutrality adjustment to balance proposed coding and payment policy changes
0.5 percent higher update for Qualified Participants (QPs) in Advanced Alternative Payment Models (APMs) under the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA)
The AMA continues to strongly advocate for annual Medicare payment updates to reflect the growth in physician practice costs as measured by the Medicare Economic Index (MEI), which CMS projects will be 2.5 percent. On July 15, Representatives John Joyce, M.D. (PA-13), Greg Murphy, M.D. (NC-03), and Kim Schrier, M.D. (WA-08), chairs of the GOP and Democratic Doctors Caucuses, introduced the Patients First Act (HR 9693), a comprehensive, bipartisan, AMA-supported MACRA reform legislation that includes an inflation-based update tied to MEI, budget neutrality reform, a MIPS replacement, APM reforms, and a new primary care payment pilot that would not impact budget neutrality.
In its 2026 report, the Medicare Payment Advisory Commission (MedPAC) recommended increasing payment rates for physician services “to bring fee for service Medicare’s overall payment levels closer in line with providers’ costs.” The 2026 Medicare Trustees Report likewise warned MACRA “raises important long-range concerns that will almost certainly need to be addressed by future legislation… physician payment updates …do not vary based on underlying economic conditions, nor are they expected to keep pace with …physician cost increases… Absent a change in the delivery system or level of update by subsequent legislation, the Trustees expect access to Medicare-participating physicians to become a significant issue in the long term.”
Practice Expense (PE) Methodology – Newly Proposed Changes
In response to the AMA’s previous request, CMS published the algorithm utilized to calculate PE relative value units (RVUs) to promote transparency. CMS proposes the following changes effective Jan. 1, 2027:
Allocate indirect practice expense based on both physician work RVUs and clinical labor for all services except 10- and 90-day global period codes. CMS does not provide a rationale for excluding 10- and 90-day global codes, which would be disadvantaged in any redistribution that results from this change.
Simplify the methodology by removing the indirect practice cost indices (IPCI) from the calculation of the practice expense RVUs over a two-year transition period. The specialty level IPCIs are published on the CMS website and vary from 0.6 to 2.2. This modification would result in specialty redistribution.
Introduce a stabilization adjustment to practice expense RVUs to ensure services not otherwise modified (new, revised or revalued) are not impacted in practice expense adjustments by more than five percent relative to the previous year. This stabilization adjustment will occur prior to the statutory phase-in, which limits all codes that are not new or revised to a 19 percent decrease in total RVUs in a given year.
Medicare Economic Index (MEI)
CMS proposes to continue the MEI cost shares for physician work, PE, and professional liability insurance for 2027, which the AMA supports. A previous CMS alternative would have resulted in a significant decrease in the proportion of physician payment allocated to physician work and was opposed by organized medicine.
Update to Practice Expense Site of Service Payment Differential
In 2026, CMS implemented a controversial methodology change to reduce the indirect practice expense payment for all services provided in the facility setting, citing concern that duplicative payments were made between the physician and hospital payment systems. CMS reduced the portion of facility practice expense RVUs allocated based on work RVUs to half the amount allocated to non-facility PE RVUs. This resulted in a seven percent cut to facility-based payment, while non-facility-based payment to physicians increased by four percent. Resulting payment changes to individual physicians and specialties were substantial. The AMA pushed back strongly against the proposal and called for CMS to make changes based on reviewing individual services, rather than broad disruptive policies, highlighting the results of our Physician Practice Information Survey.
In this proposed rule, CMS acknowledges “unintended, but significant” issues that resulted from this policy. The Agency proposes to address one particular anomaly to ensure that nursing facility visit payments will again be equalized in 2027. CMS further states that there are ongoing concerns with the policy as the “current binary of facility and non-facility does not account for the range of employment models associated with physician services that drive significant differences in actual practice expenses.” CMS requests comment on alternatives, including a percentage less than 50 percent; utilizing a new modifier to identify employed physicians to isolate payment reductions; or other methods to address their concern about duplicative practice expense payment.
Strategies to Improve Payment Transparency, Accuracy, and Congruency Across Payment Systems
Professional and Technical Components
A file is posted to the CMS website that displays the non-facility (office) practice expense RVUs and the facility practice expense RVUs, labeling facility RVUs as “26 – professional” and the difference between the non-facility and facility RVU as “TC-technical.” CMS states that it is sharing this information to provide transparency and to “facilitate more consistent comparisons across services and settings.” CMS requests comment on how it could use this information to assess payment differences across settings.
Global Surgical Packages
CMS continues to express concern about the accuracy of global surgery payment, specifically that post-operative visits are not being provided. This hypothesis is largely derived from a flawed attempt to require some physicians to report non-covered CPT code 99024 Postoperative follow-up visit, normally included in the surgical package, toindicate that an evaluation and management service was performed during a postoperative period for a reason(s)related to the original procedure for certain services. The AMA has previously detailed the concern with this data collection effort and resulting CMS analyses, beginning on page 31 of the AMA comment letter on the 2022 PFS proposed rule. CMS now proposes to pause the data collection effort for CPT code 99024, citing undue burden to physicians. However, the Agency requests comment on whether the CPT code 99024 reporting requirement should be expanded to all physicians or if other data sources are available to demonstrate the number of visits provided. An Excel file is posted to the CMS website that computes relative values without the post-operative visits for all 10- and 90-day global period services and CMS also calls for comment on potential revaluation strategies to consider in future rulemaking.
Valuation of Specific Codes
CMS proposes to accept 88 percent of the AMA/Specialty Society RVS Update Committee (RUC) recommendations and 100 percent of the RUC Health Care Professionals Advisory Committee (HCPAC) Review Board recommendations for new/revised CPT codes and codes identified via the RUC’s potentially misvalued services process. CMS also proposes to accept nearly 100 percent of the AMA’s direct PE recommendations. CPT 2027 will include a major restructuring of maternity care services and speech-language pathology services, and several other coding and payment changes ranging from prostate biopsy to magnetic resonance angiography – head and neck.
Maternity Care Services
The AMA is pleased that CMS adopted AMA’s recommendations to update the Maternity Care Services coding structure. Beginning January 1, 2027, the CPT codes will be updated to comprehensively revise the maternity codes, reflecting modern obstetric practice. The new code structure will provide much needed transparency for patients, and the increased granularity will improve the ability of physicians and researchers to better understand the drivers of maternal mortality. The AMA believes CMS’ solicitation for comments on maintaining current coding through the creation of HCPCS G-codes will create unnecessary confusion and urges CMS to finalize the Maternity Care Services CPT code set without maintaining the historical global structure via HCPCS G-codes.
Remote Monitoring
CMS began payment of CPT codes for remote physiologic monitoring (RPM) in 2019. Codes for remote therapy monitoring (RTM) followed, as well as expansion of coding for RPM. CMS has required that RPM services be furnished only to established patients since 2021. For 2027, CMS proposes that RTM services also be furnished only to established patients. Clinicians reporting RPM or RTM services must furnish a separately reportable initiating visit in association with the onset of RPM or RTM services. For 2027, CMS is proposing to only allow payment for RPM or RTM services when performed by clinical staff employed by the practice and not when those services are delivered by contractors.
Citing their belief that a lack of data regarding the typical device used in the provision of RPM and RTM services has led to possible overpayment, CMS proposes to decrease the PE RVUs for several of these services using crosswalks to other services and eliminating all direct practice costs for the treatment management codes. These changes will result in significant payment reductions in RPM and RTM services in 2027.
As payment reductions are limited to 19 percent per year, several of these codes will continue to be reduced in future years until CMS’ proposed values are fully implemented. However, CMS is not bound by the 19 percent reduction for new codes. Accordingly, CMS proposes bundling the RPM and RTM CPT codes and creating four new HCPCS G-Codes in 2027 to describe remote monitoring services, which would lead to immediate implementation of significant cuts to the monthly supply codes.
The RUC is scheduled to re-examine the RPM codes in January 2028 and determine if the RTM codes need to be examined in 2030 after claims data are available.
Evaluation and Management (E/M) Visit Complexity Add-On (HCPCS Code G2211)
CMS proposes to replace E/M Visit Complexity add-on HCPCS code G2211 with a modifier referred to as MOD1. CMS believes that the resource costs of furnishing longitudinal care for beneficiaries are not best characterized as a separate service and code. Rather, CMS believes that since the work is an inherent part of the visit, it would be more accurately valued as a modifier to the base E/M code. MOD1 would be reported under the same circumstances that HCPCS code G2211 is reported now with a slightly different descriptor: Visit complexity inherentto new or established office/outpatient or home or residence evaluation and management service, associated withmedical care services that serve as the continuing focal point for all needed health care services and/or with medicalcare services that are part of ongoing care related to a patient’s single, serious condition or a complex condition. CMS proposes payment for MOD1 as 16 percent of the E/M base code using a weighted average of the percentage increase that G2211 comprised relative to two office or other outpatient visit E/M codes, weighted by utilization, and adjusted for budget neutrality. The Agency would also create a separate modifier MOD2 to be exclusively available to Accountable Care Organization (ACO) participants, paid at 32 percent of the E/M base code.
Additional Newly Covered Services
CMS is proposing to create G codes and cover a number of new services in 2027, including: shared medical visits; advance care planning by clinical staff; vaccine adverse effects management; health coaches; and vascular embolization or occlusion procedure with use of a pressure-generating catheter.
Accounting for E/M Resource Overlap Between Stand-Alone Visits and Global Periods
CMS proposes to change payment for services using Modifier -25 Significant, Separately Identifiable Evaluation andManagement Service by the Same Physician or Other Qualified Health Care Professional on the Same Day of theProcedure or Other Service. CMS proposes to reduce payment when a separately identifiable E/M office visit is furnished by the same physician (or a physician in the same group practice) on the same day as a 0-, 10-, or 90-day global procedure. Under this proposal, the most expensive service (either surgical or E/M visit) would be paid 100 percent, and all other surgical procedure(s) or E/M visit(s) would be paid at 50 percent. The AMA will vigorously oppose this policy as the procedure codes most impacted by this proposal have already been valued to only include the work and resource costs that are above and beyond the E/M office visit. This proposal is inherently unfair to office-based physicians who perform minor procedures in their office. CMS is also seeking comment on how this policy might apply to an E/M visit reported on the same day as CPT code 67028 Intravitreal injection of apharmacologic agent.
Software as a Medical Service (SaMS) Laboratory Analyses
CMS proposes a change in terminology from Software as a Service (SaaS) to Software as a Medical Service (SaMS). SaMS will refer to software-based technologies that support clinical decision making through algorithmic analysis, including those that provide clinical or diagnostic functionality.
CMS takes the position that a SaMS should be treated the same way whether its algorithm analyzes an imaging test (e.g. a CT scan) or data produced by a laboratory test. In its view, all such algorithmic analyses are comparable to other SaMS analyses and fall within the broader proposed framework for SaMS. CMS expects that applying this consistent approach to SaMS technologies would support stability and predictability in payment for similar services.
Accordingly, for CY 2027, CMS is proposing to contractor price ten HCPCS codes that describe various SaMS analyses performed on laboratory tests under the PFS. These ten codes were identified using each code’s CPT descriptor. Where a descriptor included no laboratory method and described only a computer analysis, CMS classified the code as a SaMS analysis performed on laboratory tests. CMS solicits comments on the ten-code proposal and any other SaMS analysis performed on lab tests that should be removed from the Clinical Laboratory Fee Schedule (CLFS) and contractor priced under the PFS, as well as input on approaches to payment for these services.
Potentially Misvalued Services
The positive budget neutrality RVU adjustment is partially due to the savings produced from the RUC’s identification and review of potentially misvalued services. For 2027, CMS received 13 nominations identifying potentially misvalued services for future review. CMS reviewed these comments and welcomes additional comments and review by the RUC on several areas.
Medicare Telehealth Services
CMS did not receive any requests for additions to the Medicare Telehealth List, but proposes to add several of the new services mentioned above to this list: advance care planning services provided by clinical staff under the direction of the treating physician; group-based medical sessions; treatment of speech and certain other disorders for pediatric patients; and visits to diagnose and treat vaccine adverse effects.
The Consolidated Appropriations Act (CAA), 2026, extended flexibilities that allow Medicare telehealth services to be delivered nationwide and patients to receive services in their homes through 2027. Audio-only services are also extended, and in-person visit requirements for telehealth for mental health services are delayed through 2027. The CAA 2026 also requires CMS to create modifiers for telehealth furnished through a virtual telehealth platform by a physician who contracts with or has a payment arrangement with an entity that owns the platform. CMS establishes modifiers BB and BC for this purpose. CMS also proposes changing the G-codes for telehealth critical care to mirror the two CPT codes for critical care, so there will now be G-codes for the first 30 to 74 minutes and for each additional 30 minutes.
Finally, CMS is changing its policy on teaching physicians providing virtual supervision of residents. The current policy requires that the teaching physician, resident, and patient be in three different locations. The new policy will allow teaching physicians to bill for services involving residents when either the teaching physician or the resident is in the same physical location as the patient.
Outpatient Rehab Facility Services and KX Modifier Thresholds
CMS proposes routine and technical changes, including technical corrections to fix outdated cross-references and the statutorily required annual inflation update to the KX modifier thresholds (formerly known as therapy caps), which would increase from $2,480 to $2,540 for CY 2027 based on a proposed MEI update of 2.5 percent. The KX modifier thresholds would be updated in the final rule using more recent MEI data. The targeted medical review threshold remains at $3,000 through CY 2027, as set by statute, and will begin receiving annual MEI-based updates in CY 2028.
Supporting Beneficiaries Planning for Future Medical Decisions (Advance Care Planning Services)
CMS proposes two new HCPCS codes for advance care planning (ACP) services provided by clinical staff under the direct supervision of a physician or other qualified health professional. The existing ACP codes would be limited to time personally spent by the billing practitioner. The proposal reflects growing recognition that ACP is a longitudinal, team-based service and could help practices incorporate these conversations more routinely into ongoing care, expand patient access, and preserve physician involvement when clinical expertise is required.
Rural Health Centers (RHCs) and Federally Qualified Health Centers (FQHCs)
CMS proposes to recognize diabetes self-management training (DSMT) and medical nutrition therapy (MNT) as stand-alone billable RHC visits paid at the all-inclusive rate, provided the services are furnished by a certified provider under the direct supervision of RHC professional staff. Currently, these services are not separately payable when furnished during an RHC encounter, and CMS cites low utilization as justification (in 2024, DSMT reached just 0.005 percent of RHC beneficiaries, with utilization rates 22 times higher in FQHCs and 17 times higher in rural physician offices). As in FQHCs, if DSMT or MNT is furnished on the same day as another qualifying visit, the RHC would be paid at a single per-visit rate. CMS states that it does not expect to propose additional preventive services beyond those already payable in FQHCs and physician offices.
CMS proposes other routine updates for CY 2027 including the annual FQHC prospective payment system market basket update of 2.5 percent, which would raise the base payment rate from $207.72 to $212.91 (to be updated in the final rule using more recent MEI data), as well as other conforming regulatory text changes.
Proposed Changes to the Ambulatory Specialty Model (ASM)
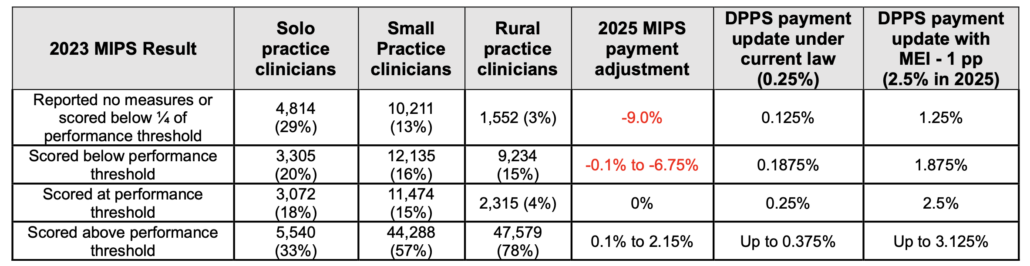
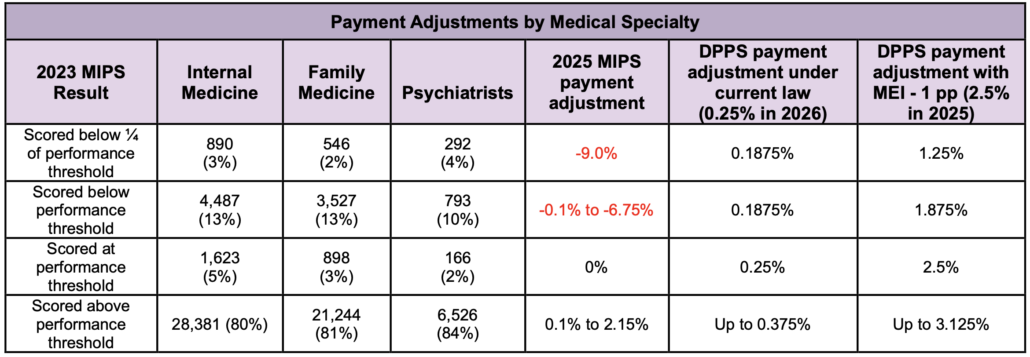
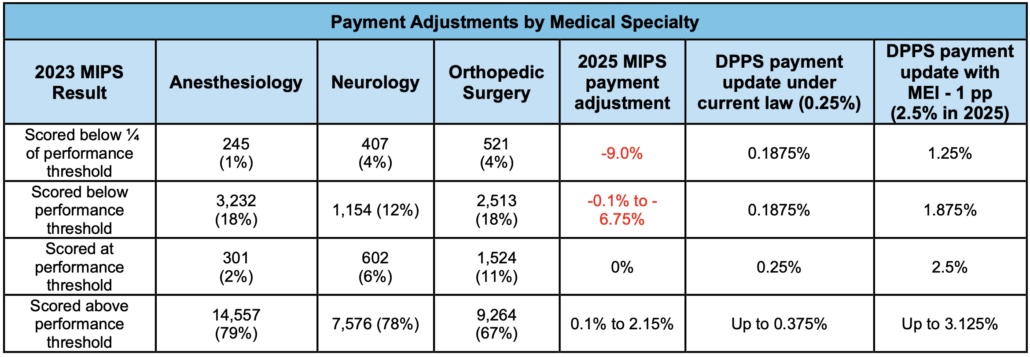
In 2026, CMS finalized ASM as a mandatory payment model that will run for five years beginning in 2027. Several types of specialists in 240 geographic areas will be required to participate: (1) cardiologists who deliver services to 20 or more patients with heart failure, and (2) anesthesiologists, pain management physicians, neurosurgeons, orthopedic surgeons, and physiatrists who deliver services to 20 or more patients with low back pain. Beginning in 2029, specialists participating in ASM will face payment adjustments based on their ASM scores from two years earlier of +/- 9%, growing to +/- 12% by 2033. These scores will be based on participants’ performance on measures relative to other physicians in ASM.
CMS is proposing to make a number of “technical refinements and adjustments,” several of which are responsive to the AMA’s prior recommendations, including:
A specialty group practice would be permitted to have a single Collaborative Care Agreement (CCA) with a primary care practice that covers all the specialists in the group, rather than every individual specialist in the group being required to have their own separate CCA with that practice.
Cardiologists could be exempted from ASM if they notify CMS that their primary specialty is cardiac electrophysiology, cardiac surgery, interventional cardiology, advanced heart failure and transplant cardiology, or adult congenital heart disease rather than general cardiology. The AMA objected to having specialty determinations made by CMS based on out-of-date or inaccurate information, which led to inappropriately including subspecialists.
The Functional Status Change for Patients with Low Back Impairments measure would be removed and replaced with the Functional Outcome Assessment measure, which would measure whether functional outcome assessments are conducted, rather than attempting to determine whether functional status has improved.
CMS proposed several AMA-sought revisions to Promoting Interoperability (PI) requirements for ASM participants to reduce reporting burden. Specifically, a separate attestation to completing a security risk analysis would no longer be required; the Office of the National Coordinator for Health Information Technology (ONC) Direct Review and ONC-Authorized Certification Body (ACB) Surveillance attestations would be removed; and the Electronic Prior Authorization (ePA) measure would be optional (and unscored) for 2027. These changes align with those proposed in the MIPS PI Category.
Unfortunately, other proposed ASM changes are potentially burdensome or problematic, including:
Performance scores for physicians practicing in a rural area (regardless of their practice size) would be increased by five points (i.e., 5 percent). Because of the tournament structure of ASM, this could make it more likely non-rural physicians receive a payment reduction despite good quality performance.Performance scores would be increased by five points (i.e., 5 percent) if a physician voluntarily submits patient-reported outcome data and risk adjustment data in a manner specified by CMS. However, CMS has left this largely undefined. Larger and better-resourced practices may be more equipped to receive these additional points, which could negatively impact physicians in small and independent practices.
Administrative claims-based quality measures would be calculated at the individual level, even if a small practice reports quality measures as a group, which could penalize physicians focused on complex patients.
A modified version of the Magnetic Resonance Imaging of Lumbar Spine for Low Back Pain measure would be added back into the low back pain component of ASM, despite previously having been removed due to concerns from the AMA and other stakeholders. The proposed new measure would attribute an MRI to any physician who delivered other low back pain-related services to a patient up to a year prior.
Despite the AMA’s strong opposition, ASM would remain a mandatory model.
The model design continues to use a “redistribution percentage” of 85 percent, which guarantees that the majority of participating physicians will receive a reduction in their Medicare payments regardless of how well they perform on the measures. The AMA recommended increasing the percentage to 100 percent.
Physicians would be rewarded or penalized based on whether their performance score is higher or lower than the scores received by the other physicians in ASM during the same year. The AMA recommended setting performance thresholds in advance so physicians know what they need to do to avoid a penalty.
CMS would also only provide performance feedback after the performance year has ended.
Unlike other models in which downside risk is phased in over time, physicians in ASM could see their payments cut by up to 9 percent during the first year of the program. The AMA recommended reducing the maximum risk level in the initial two years to two percent.
Physicians treating as few as 20 relevant patients would be required to participate, even if ASM patients are a small subset of their patients. The AMA recommended a higher threshold.
No additional points would be awarded for improved quality and spending performance.
The AMA remains concerned that the proposed quality measures would not accurately or adequately assess whether Medicare beneficiaries had achieved better outcomes nor prevent patient safety concerns, while the cost measures could penalize physicians for aspects of spending they cannot control, such as when services are ordered by other specialists, or when drug prices increase.
No additional payments would be provided to support enhanced preventive care, coordination with primary care physicians, care management, and other services that could improve outcomes for ASM patients.
CMS indicated that it was exploring “whether including additional conditions and specialists would be appropriate,” although it did not propose any expansion of the model in this proposed rule.
Limiting Medicare Coverage of Certain Individuals
The proposed rule would add a new Medicare specific definition of “eligible noncitizen.” Specifically, an “eligible noncitizen” would be an individual who is (1) an alien lawfully admitted for permanent residence under the Immigration and Nationality Act; (2) an alien who has been granted the status of a Cuban or Haitian Entrant, as defined in section 501(e) of the Refugee Education Assistance Act of 1980 (Pub. L. 96-422); or (3) an individual who lawfully resides in the United States in accordance with a Compact of Free Association (COFA) referred to in 8 U.S.C. 1612(b)(2)(G). The rule expressly states noncitizen U.S. nationals who are eligible for Medicare under section 1899C(a)(1) of the Act would no longer be considered “eligible noncitizens.” However, legal permanent residents who meet the five-year continuous residency requirement and other applicable Medicare requirements would maintain their Medicare benefit. On January 1, 2027, individuals that do not meet the proposed revised definition of an “eligible noncitizen” would no longer be able to obtain benefits under Medicare. CMS includes a proposed termination, enrollment, and notification framework to implement these changes.
Medicare Shared Savings Program (SSP)
This year’s rule includes myriad SSP changes, mainly to increase beneficiary enrollment, reduce administrative burden on ACOs, and make the program more “efficient,” i.e. reduce federal payouts to ACOs. CMS predicts that collectively, these changes will reduce SSP outlays by $5.5 billion over the next decade.
For beneficiary assignment, CMS proposes to exclude allowed charges for primary care services billed through a non-ACO TIN and slightly loosen eligibility criteria pertaining to Medicare enrollment status starting in performance year 2028 (PY 2028). Both changes are expected to slightly increase the number of assignable ACO beneficiaries for the vast majority of ACOs, with a larger impact on a select few. Because these newly assignable beneficiaries are anticipated to have higher costs and be more medically complex, these changes are anticipated to negatively impact gross savings/losses. In addition, CMS proposes to add the following services to the list of primary care services used for assignment: screening, brief intervention, referral to treatment, vaccine adverse effects management, and Advance Care Planning.
Regarding financial methodologies, CMS proposes changes aimed at “recalibrating incentives” between the BASIC and ENHANCED tracks to ensure ACOs do not advance to higher levels of risk too quickly, then drop out.
Specifically, CMS proposes to increase the sharing rate for ACOs in BASIC Level E from 50 to 60 percent and tolower the maximum positive regional adjustments for ENHANCED ACOs from 50 to 35 percent. CMS also proposes to increase the prior savings adjustment from 50 to 75 percent to encourage continued participation by existing ACOs. To incentivize ACOs to expand into new participating practices and beneficiary populations, CMS proposes to add a new “growth adjustment factor” that would be applied on top of the existing adjustment factors (up to the cap). CMS also proposes to risk-adjust the five percent benchmark adjustment cap to allow ACOs with complex patient populations to more fully benefit from benchmark adjustments. All these changes would apply to new agreement periods starting in 2027 or later. CMS proposes to adjust the Accountable Care Prospective Trend (ACPT) component of the benchmark update factor on an annual basis and to apply the same annual rate to all ACOs regardless of start date to promote consistency across cohorts. CMS would apply guardrails to mitigate large fluctuations. Lastly, CMS proposes to replace the visit complexity add-on code G2211 with modifiers that would reimburse physicians at 32 percent of the E/M base code for ACO participants, twice the amount as for non-ACO participating physicians.
CMS proposes to discontinue prepaid shared savings due to limited uptake in 2026, the first year they were available. Uptake was limited due to strict guardrails overqualified spending categories and mandatory itemized spend plans. Out of 23 ACOs that applied, only four were approved. AMA plans to push back on this proposal and reiterate previous asks to loosen restrictions on this funding.
CMS intends to improve the accuracy of advance investment payment calculations by adding a rural component and replacing Area Deprivation Index with a flat per beneficiary rate for non-rural, non-Low-Income Subsidy/dually eligible beneficiaries starting in PY 2028.
This year’s rule includes substantial quality reporting changes for SSP ACOs, many of which align with long- standing AMA asks, including extending the availability of the MIPS clinical quality measure (CQM) collection type, establishing Medicare electronic CQMs (eCQMs) as a collection type (in addition to Medicare CQMs), amending MIPS data completeness requirements, updates to the APP Plus quality measure set, applying flat benchmarks to measures reported through Medicare CQMs and Medicare eCQMs, and revising scoring policies for excluded measures and non-benchmarked measures. CMS proposes several changes to the APP Plus quality measure set for SSP ACOs, including the removal of Initiation and Engagement of Substance Use Disorder Treatment (Quality ID: 305) and Adult Immunization Status (Quality ID: 493), which the AMA supports. The APP Plus quality measure set would include a total of eight measures in PY 2027, including five eCQMs/MIPS CQMs/Medicare CQMs/Medicare eCQMs; two administrative claims-based measures; and the Consumer Assessment of Healthcare Providers and Systems (CAHPS) for MIPS survey measure.
In response to unified stakeholder opposition led by the AMA and other stakeholders, CMS proposes to reverse its previously finalized change from the 2024 PFS final rule that SSP ACO participants, regardless of track or Advanced APM QP status, must report all MIPS PI measures in order to satisfy SSP CEHRT use requirements. Instead, CMS proposes to allow SSP ACO participants to satisfy CEHRT use requirements through one of the following three flexible options: 1) successfully report at least one ACO-reported measure in the APP Plus quality measure set through eCQMs or Medicare eCQMs; 2) attest to using Fast Healthcare Interoperability Resources (FHIR) capabilities in certified health IT to support reporting of at least one ACO-reported measure; or 3) attest to one of three ACO CEHRT use metrics, a longtime AMA ask.
In another victory for AMA advocacy, CMS proposes to reverse another burdensome previously-finalized requirement that every ACO provider/supplier in the ACO must successfully report on a PI measure for an ACO to satisfy CEHRT use requirements. Instead, ACOs would be allowed to attest “Yes” to CEHRT use metrics for purposes of satisfying CEHRT use requirements if at least one ACO provider/supplier in each of the ACO’s participating TINs performed the relevant action, with certain exclusions for those with special status, a MIPS exception, or a hardship exception. CMS also proposes to extend enforcement discretion related to these proposals through the 2026 performance year so that failure to satisfy PI requirements will not negatively impact an ACO’s shared savings or losses. CMS does clarify that SSP ACO participants that are not Qualified Advanced APM Participants will still be required to report PI measures (unless they are otherwise excluded) for purposes of MIPS participation as before.
Effective Jan. 1, 2027, CMS proposes to revise beneficiary notification requirements to reduce operational burden on ACOs. Specifically, timing for initial beneficiary notification requirements would be a set date that aligns with the ACO REACH Program, rather than prior to or at the first primary care service visit. CMS also proposes to eliminate the beneficiary follow-up communication requirement, citing a lack of evidence that it improves beneficiaries’ understanding of ACOs or value-based care. Lastly, CMS proposes to allow ACOs to elect to reduce or waive beneficiary cost sharing for certain services, including deductibles and/or coinsurance amounts. Applications would be collected in early 2027 and applied by a target date of April 1, 2027.
Clinical Laboratory Fee Schedule
CMS is proposing conforming regulatory changes to implement statutory amendments to the Protecting Access to Medicare Act of 2014 (PAMA) enacted in CAA, 2026, specifically data reporting and payment phase-in requirements including use of 2025 private payor data to establish updated CLFS rates beginning in 2027 and annual payment reductions of no more than 15 percent through 2029. These changes do not address underlying structural issues in the PAMA methodology, including concerns about whether the reported data adequately represent physician-office, hospital outreach, rural, and other laboratories. CMS cannot alter the statutory methodology through rulemaking; Congress must act to permanently reform PAMA and address potential payment reductions. AMA is actively working in concert with multiple stakeholders on a Congressional fix.
II. QUALITY PAYMENT PROGRAM (QPP) PROVISIONS
Merit-based Incentive Payment System (MIPS)
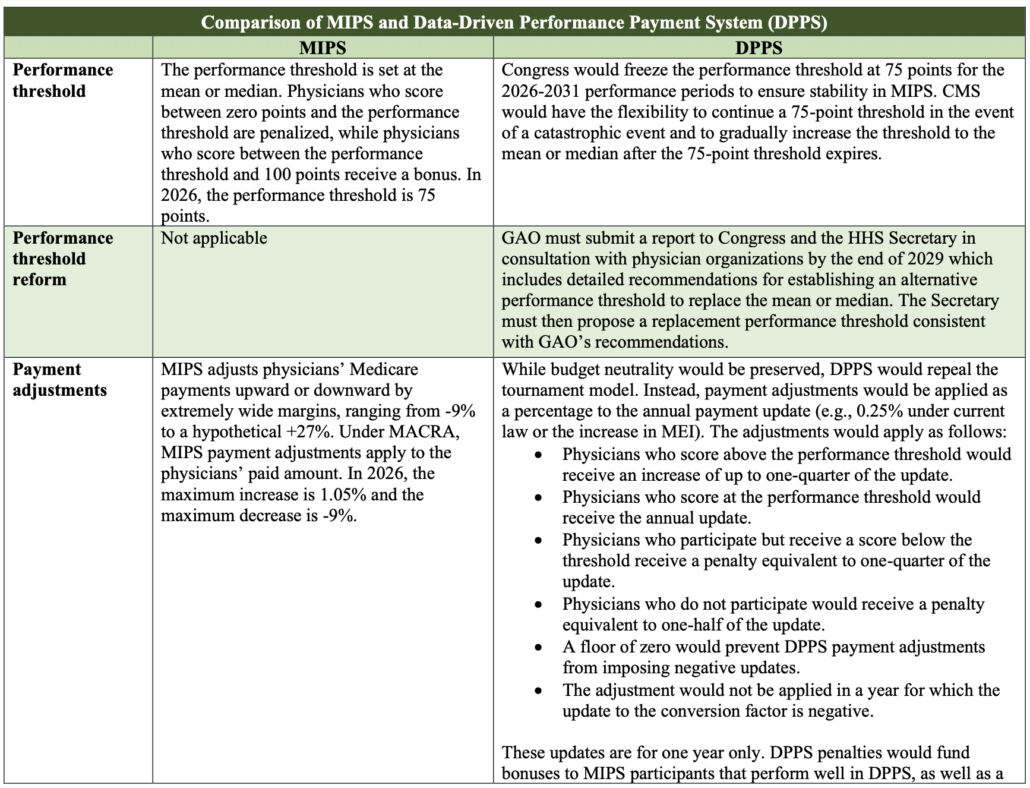
Following ongoing advocacy by the AMA, last year CMS finalized policy to maintain the threshold to avoid a MIP penalty at 75 points through the CY 2028 performance year/2030 MIPS payment year.
MIPS Value Pathways (MVPs)
Despite strong objections by the AMA, CMS has proposed to sunset traditional MIPS and transition to MVPs in 2029. CMS is proposing to expand the MVP portfolio to include Diabetic Disease, Hypertension and Hospitalist MVPs starting with PY 2027. In addition, CMS is proposing to modify all 27 existing MVPs to include MIPS core measure selections for each MVP, add measures that expand upon a clinical concept or capture additional specialties most applicable to report an MVP, address maintenance requests from the public, and remove measures and activities that would either be finalized for removal from their respective MIPS inventory or replaced by more robust measures. In addition, CMS is proposing to rename the Rehabilitative Support for Musculoskeletal Care MVP to Rehabilitative Support MVP. Furthermore, CMS is proposing that virtual groups would be able to report an MVP beginning with in PY 2029. Despite AMA support, CMS proposes to rescind its policy to not publicly report any MVP data any new Improvement Activity or Promoting Interoperability measure, objective, or activity during the first year it is included in an MVP.
Quality
Starting with PY 2027, CMS is proposing to replace the outcome / high-priority measure reporting requirement in traditional MIPS and MVPs with a MIPS core measure reporting requirement. Eligible clinicians or group practices would have to report a core measure as one of their six measures in MIPS or as one of their four measures in an MVP. Small practices would be exempt from this requirement. Any eligible clinician, group, virtual group, subgroup, or APM entity that does not report a MIPS core measure and is not a small practice would receive zero points for one of their required measures unless they submitted an attestation that they did not have an applicable MIPS core measure and submitted another measure in its place. CMS has proposed to designate 78 MIPS quality measures, many of which were previously designated as outcome/high priority. In general, the AMA has not been supportive of the outcome measure requirement or moving to core measures, as measurement should be based on what is most appropriate for a physician’s scope of practice or following an episode of care, not arbitrary metrics and reporting for the sake of reporting.
Beginning with PY 2027, topped out MIPS core measures subject to the seven-point scoring cap (i.e., those topped out for two or more consecutive performance periods) would no longer be subject to that cap and would instead be scored according to the defined topped out measure benchmark (with a 10-point maximum). CMS has proposed to designate 17 measures as topped out but with the defined measure benchmark and not subject to the seven-point scoring cap due to limited measure choice.
CMS also proposes a number of changes to the PY 2027 quality measure inventory including removing 20 existing quality measures, adding 10 new measures, and substantive changes to 43 quality measures, all of which are summarized in Appendix 1. Qualified Clinical Data Registry (QCDR) measures are not included in Appendix 1 because they are subject to a separate review process.
Cost
CMS does not propose to adopt any new, remove any existing, or propose substantive changes to any existing MIPS cost measures for the 2027 performance year. However, CMS proposes non-substantive updates to the list of care episode and patient condition codes to reflect coding changes, summarized here. The AMA will continue to advocate for more targeted and clinically relevant cost measures.
Promoting Interoperability (PI)
In response to longstanding AMA advocacy, CMS proposes several changes to the MIPS PI category to reduce administrative burden and focus on high-value, outcome-oriented measures. Specifically, CMS proposes to update the definition of CEHRT to align with ONC’s changing Health IT Certification Program, remove the ONC Direct Review and the optional ONC-ACB Surveillance attestations retroactive to the CY 2026 performance year, and remove the Security Risk Analysis measure to reduce redundancy, as security risk analysis and risk management activities are already separately required under the HIPAA Security Rule.
CMS proposes to make the previously finalized electronic prior authorization measure optional for the 2027 performance year, with an opportunity to earn 10 bonus points. The attestation-based measure would then become mandatory in 2028. CMS proposes more explicit technology requirements, including use of ONC CEHRT, and use of CEHRT that includes health IT certified to all three ONC ePA criteria.
Lastly, CMS proposes a new attestation-based electronic prior authorization (ePA) for prescription drugs measure to assess utilization of standards-based ePA. For PY 2028, CMS proposes that a MIPS-eligible clinician attest to having requested PA electronically using CEHRT for at least one prescription drug ordered. There are several proposed exclusions, including clinicians that do not prescribe drugs that require PA. A summary of proposed requirements for the PI Category can be found in Table C-G 6.
Improvement Activities
CMS proposes various updates to the inventory of improvement activities, including adding six new, modifying five, and removing 11 activities. These changes are summarized in Appendix 2.
Advanced APMs
CMS proposes to apply Qualifying APM Participant (QP) status and Partial MIPS-eligible at the TIN/NPI combination level. Any APM-related financial incentives, including APM Incentive Payments and the QP conversion factor differential, would apply only to claims associated with Advanced APM-participating TINs. CMS says this will “prevent an increasing windfall for TINs that do not participate in Advanced APMs, particularly given that the higher qualifying conversion factor update.” The agency estimates that “relatively few QPs would be affected” because the majority of QPs are participating in an Advanced APM through all TINs. CMS estimates that this change would result in approximately $2.38 billion less being paid out to APM participants over the next decade.
CAA 2026 reinstated the APM Incentive Payment for payment year 2028 (based on 2026 performance) at 3.1 percent. Absent further congressional action, the APM incentive payment will expire at the end of the 2026 performance year/2028 payment year. The QP thresholds are also set to increase from 50 to 75 percent of Medicare payments, and from 35 to 50 percent of Medicare patients. The AMA continues to advocate for Congress to extend the APM incentive payment, freeze the QP thresholds, and to adopt permanent flexibility for the Secretary to adjust QP thresholds as needed. The latter two are included in the Patients First Act.
III. REQUESTS FOR INFORMATION (RFIs)
CMS included several RFIs in the proposed rule, including one that targets the CPT code set and the processes used to develop and value it, and another that takes a broader look at primary care payment, signaling CMS may be considering more significant changes in the future, as explained further below.
Current Procedural Terminology (CPT) RFI
CMS includes an RFI examining the AMA’s CPT coding system, CPT licensing, the CPT code development process, and the RUC. The RFI asks about alleged harms associated with the AMA’s “monopoly over CPT-4 licenses” and cites concerns about reliance on a private organization with an “obvious conflict of interest” in recommending physician service values, seeking input on CPT licensing costs and effects, the role of medical necessity in code development, possible alternatives or supplements to CPT as the national physician services code set, alternative governance and valuation processes, and whether physician services could instead be paid using ICD-10-PCS or other bundled payment approaches.
Redesigning Primary Care to Make America Healthy Again
CMS is seeking comment on a broad reexamination of how Medicare pays for primary care, with the goal of better supporting prevention, longitudinal care, and practice transformation. Specifically, CMS is requesting feedback on three areas: (1) whether the PFS appropriately values primary care services relative to other services; (2) how payment policies should evolve to account for the growing role of technology in delivering primary care; and (3) whether Medicare should transition from traditional fee-for-service payment toward prospective, population-based payments or outcomes-based payments for primary care, beginning with the Medicare SSP and potentially expanding more broadly across Original Medicare. The RFI reflects an important shift in CMS’ thinking about primary care payment signaling it may place greater emphasis on longitudinal accountability for patient outcomes, rather than reimbursement for discrete visits and services in the future.
Other RFIs (In order of appearance)
Community-based palliative care (page 108)
Intensive lifestyle interventions to slow progression of Alzheimer’s Disease (page 109)
Applying electronic prior authorization measures to SSP ACOs (page 225)
Specialty care in the SSP (page 287)
Duplicate laboratory testing, imaging, and result sharing and interoperability (page 298)
Fast Healthcare Interoperability Resources (FHIR) (page 302)
FHIR-Based Digital Quality Measurement in the QPP and Other CMS Quality Programs (page 310)
Future Potential Performance-Based Measures of Electronic Prior Authorization (page 341)
MVP scoring (page 365)
Star Rating Assignment Methodology for Administrative Claims Quality Measures (page 373)
Cyclosporiasis is an infection of the intestine caused by a parasite called Cyclospora (SIGH-clo-SPORE-uh). Cyclosporiasis is not spread directly from person-to-person. Infected people pass Cyclospora in their feces (stool), but this form of the parasite cannot make people sick. The parasite needs time (days to weeks) in the environment to change into a form that can make people sick. This form of the parasite then can infect someone by entering the body through the mouth, typically by eating or drinking something that is contaminated with Cyclospora. Cyclosporiasis usually causes watery diarrhea with frequent, sometimes explosive, bowel movements. Other symptoms can include loss of appetite, weight loss, bloating, increased gas, stomach cramps, nausea, vomiting, muscle aches, low-grade fever, and fatigue. Some people who are infected with Cyclospora do not have any symptoms. Symptoms usually appear within one week after exposure. Past outbreaks of cyclosporiasis in the United States have been linked to imported fresh produce, such as raspberries, basil, lettuce, and snow peas. The produce involved in each outbreak was probably contaminated in the country where it was grown.
Several states are currently experiencing a significant increase in cases of cyclosporiasis and some have detected outbreaks. States are working together with federal partners to investigate these outbreaks. The investigations to identify source(s) of illness are ongoing.
The Virginia Department of Health (VDH) is closely monitoring and investigating reported cyclosporiasis cases. There is not currently evidence that Virginia is experiencing an outbreak. The number of cyclosporiasis cases reported to VDH typically increase in the spring and summer months, and are posted on the Monthly Morbidity Report.
What VDH does:
Local health districts interview ill people and gather data on when they became sick, their travel history, and foods consumed.
This epidemiologic information is then reviewed for any commonalities among cases, which is how we are able to detect food items that are potential exposure risks and potential outbreaks.
Coordinate with state and federal partners on epidemiologic investigations.
Share information with the general public when health risks are identified.
To prevent cyclosporiasis:
Wash all fruits and vegetables thoroughly under running water before eating, cutting, or cooking.
Wash hands carefully with soap and water before and after food preparation, and after using the bathroom or changing diapers.
Travelers, especially to tropical areas, should avoid eating raw or undercooked foods or drinking untreated water.
Anyone experiencing symptoms of cyclosporiasis should visit their healthcare provider. They can test for Cyclospora and prescribe the correct treatment. Physicians should report cases to their local health department. If you have been ill recently with diarrhea or vomiting or other gastrointestinal illness and believe it might be related to a restaurant or other food establishment, you can report your illness to My Meal Detective.
How resolving moral distress unlocks physicians’ potential
Burnout has become one of the defining conversations in medicine, as it should be. The pressures facing physicians and medical students are real, growing and impossible to ignore. But burnout is not the whole story.
Across medicine, many physicians are confronting something deeper: moral distress. New research shows it is widespread, distinct from burnout, and carries serious consequences for physicians, patients and the healthcare system itself. Read more.
AMA: No, physicians are not “providers”
Navigating the healthcare system is a challenge for many patients, and one reason is the system’s persistent use of confusing terminology around who is a physician. At its Annual Meeting in Chicago this week, the House of Delegates (HOD) acted to eliminate this confusion—and thereby boost patient safety—by deliberately avoiding use of the term “provider” when referring to any clinician with a medical degree.
The AMA already had policy stating that it supports requiring healthcare entities, when using the term “provider” in contracts, advertising and other communications, to specify the type of clinician being referred to by using the clinician’s recognized title, which details their education, training, license status and other recognized qualifications. The policy also supports this concept in state and federal health system reform. Read more.
More in Highlights from the 2026 AMA Annual Meeting:
What doctors want patients to know about injectable peptides
Interest in injectable peptides is rising as more people see them promoted online through health and wellness influencers for weight loss, muscle growth, recovery and anti-aging. But behind the buzz is a more important question: Are these products safe, effective and backed by evidence?
Physicians say patients should look past social media claims and marketing promises and start with a conversation with a doctor because some injectable peptides are not regulated and may carry real health risks. Read more.
https://www.msv.org/wp-content/uploads/2021/11/msv-logo_340x156.png00varmshttps://www.msv.org/wp-content/uploads/2021/11/msv-logo_340x156.pngvarms2026-06-24 17:48:052026-06-24 17:48:06Highlights from the 2026 AMA Annual Meeting: Moral distress widespread, distinct from burnout
Dr. Mollie James was embarrassed when her functional medicine practice filed for bankruptcy in 2019. She felt like a complete failure.
“I thought it was the worst thing that could happen,” James said. “I’m the ‘A’ student, the valedictorian, all those things. I didn’t want anybody to know. ”
Fast-forward seven years, and James is the owner of a multimillion-dollar concierge practice with two locations in Iowa, a third in Missouri and a fourth slated to open in Texas later this year. She also offers virtual care services.
Owning an independent practice is a daunting prospect financially. Physicians invest their savings and retirement accounts into a practice or take out business loans, but they often lack the know-how to operate a successful business. Clinics typically take years to become profitable, which may not be aviable option for doctors saddled with student loan debt.
Joining a large system or physician group that handles back-office operations and offers a steady paycheck is the easier path. However, some physicians say there is still a place for independentmedicine, despite the challenges.
Here’s what four practices have done to make it work.
Start small
James’ second act, James Clinic, launched in 2021 to treat a range of conditions through integrative medicine, including cancer, neuropathy and hormonal imbalances. It serves about 1,500 to 2,000 patients each year.
James decided to avoid past missteps and start small after the bankruptcy.
Her former practice struggled with high overhead costs. This time around, her first office in Chariton, Iowa, rented for $400 per month. James also transitioned to a self-pay model.
Branding was another hurdle to overcome. James said she developed a marketing strategy that focuses on patient needs, rather than selling products.
James wants others to avoid her mistakes. Later this year, James is launching Maverick Medical Ventures, which will support physicians who want to leave a health system and build their own practice.
Find additional income
Dr. Steve Furr, co-owner of Family Medical Clinic in Jackson, Alabama, has practiced independently for decades. His practice, which includes two other physicians and three nurse practitioners, is a designated rural health clinic.
Several years ago, the clinic launched a chronic care management program. Staff members regularly check in on patients to see if they are staying on their medications, need referrals or have any changes to report since their last appointment. Furr said the program brings in additional income and helps the clinic stay connected with patients.
Running a practice requires tough decisions, he said. Owners must assess whether patient volumes will support investments in new equipment, technology or services. In general, an investment only makes sense if the practice can at least break even on it, he said.
“As things have gotten tighter and tighter over time, you just can’t have things in your practice that you lose money on,” Furr said. “You do like any other business. You try and look and see where you can cut costs, where you can lower your overhead to try and maximize your income.”
Connect with other physicians
Dr. Stacey Bartell, owner of iTest Health Family Medicine in Livonia, Michigan, needed a change after the COVID-19 pandemic. She left a local health system in 2022 to start her practice. A decade-long stint as a medical director at a former employer meant she understood the business side of medicine.
Bartell said one of her biggest challenges is getting paid — ensuring the right codes are submitted to insurers and following up on claims denials and prior authorizations. Her practice, which serves nearly 1,500 patients, is starting to see people drop Medicaid coverage.
“There are days where I just run out of energy, ” she said. “We’re doing the best we can.” Bartell said it is helpful to collaborate with other private physicians and share resources when payment challenges arise.
Keep it lean
Dr. David Schechter built his family and sports medicine practice incrementally — developing a patient panel part time while working at other practices and teaching a residency program. He went full-time as an independent physician in 2002.
Schechter has a lean operating model. He is the sole clinician at the Los Angeles-area practice. There is one front-office employee and another employee, often a gap-year student, who takes vital signs and helps with other clinical tasks. Billing is outsourced. The practice’s expense ratio hovers at 35% to 40%, he said.
“My whole philosophy has been easing your way into private practice rather than necessarily jumping in, ” Schechter said. Schechter also specializes in chronic pain management through mind-body medicine, which attracts more patients and sets him apart from other primary care practices.
He also has reduced the number of insurance contracts and moved toward self-pay. For the remaining contracts, the practice is part of an independent physician association, which brings physicians together to increase bargaining power and secure higher reimbursement rates.
https://www.msv.org/wp-content/uploads/2021/11/msv-logo_340x156.png00varmshttps://www.msv.org/wp-content/uploads/2021/11/msv-logo_340x156.pngvarms2026-06-10 16:42:002026-06-10 16:42:52How independent physicians are making it work
The Virginia General Assembly has enacted significant amendments to Virginia’s mandatory child abuse and neglect reporting statute, Va. Code § 63.2-1509, effective July 1, 2026 (2026 Va. Acts ch. 845). The amendments tighten timelines, strengthen penalties, and impose heightened criminal liability on institutional actors — including hospitals and other facilities providing care and treatment to children – and mandatory reporters who fail to timely report suspected child abuse or neglect within 24 hours. Health care providers, hospital administrators, and compliance officers should review and update their reporting policies and training programs immediately, as appropriate, to ensure all covered employees are aware of the new requirements and penalties.
Existing Hospital Reporting Requirements for Health Professionals
For many years, Virginia law has required the Chief Executive Officer and Chief of Staff of every hospital or other health care institution in the Commonwealth to report to the Director of the Department of Health Professions (“DHP”) certain information about licensed, certified, or registered health professionals, multistate nursing privilege holders, and applicants. The primary reporting statute is summarized below; note that additional statutory reporting requirements also exist. See, e.g., Virginia Code 54.1-2909.
Hospitals are required to report to the DHP the following concerns regarding professional conduct, impairment, and disciplinary matters:
Five-day window for reporting for certain admissions: Report within five days after learning of a health professional’s involuntary admission for treatment of substance abuse or psychiatric illness. A report is also required after the 30-day period following a voluntary admission for substance abuse or psychiatric illness, unless the treating physician, physician assistant, or nurse practitioner provides written confirmation that the professional is no longer believed to be a danger to self, the public, or patients.
Thirty-day window for reporting reasonable-belief determinations: Report within 30 days after the CEO, chief of staff, director, or administrator determines, after appropriate review, investigation, or consultation with internal boards or committees, that there is a reasonable belief the health professional may have engaged in unethical, fraudulent, or unprofessional conduct.
Thirty-day window for reporting certain disciplinary proceedings: Report within 30 days after written notice to the health professional that the institution has begun a disciplinary proceeding involving intentional or negligent conduct causing or likely to cause patient injury, professional ethics, professional incompetence, moral turpitude, or substance abuse.
Thirty-day window for reporting specified disciplinary actions: Report within 30 days after written notice of disciplinary action taken during or at the conclusion of proceedings, or while under investigation, including denial or termination of employment, denial or termination of privileges, or restriction of privileges resulting from the specified categories of conduct.
Reports for resignations or privilege restrictions while under review: Report voluntary resignation from staff, voluntary restriction of privileges, or expiration of privileges while the health professional is under investigation or subject to disciplinary proceedings for matters related to patient injury risk, medical incompetence, unprofessional conduct, moral turpitude, mental or physical impairment, or substance abuse.
Required report contents and Immunity
Reports must be in writing and include the subject professional’s name, address, and date of birth; a full description of the circumstances; the names and contact information of individuals with knowledge and of individuals consulted to substantiate the facts; relevant medical records when patient care or the professional’s health status is at issue; and notice if the hospital has submitted an NPDB report. The health professional must be provided a copy of the report. Good-faith reporters and participants in related investigations or proceedings receive civil immunity absent bad faith or malicious intent. However, immunity is a defense that must be proven, and it does not bar a lawsuit from being filed. Failure to make a required report may result in a civil penalty of up to $25,000 and may affect licensure, certification, or renewal until the penalty is paid.
Peer review privilege preserved
Compliance with the reporting statute does not waive or limit Virginia’s peer review privilege under Va. Code § 8.01-581.17. The privilege does not bar required reports or requested medical records necessary to investigate reportable unprofessional conduct but privileged materials may be withheld. Hospitals and health systems should confirm that their practitioner health, medical staff, credentialing, peer review, human resources, and compliance processes identify when a matter triggers reporting under Va. Code § 54.1-2400.6 and other reporting statutes, in addition to the child abuse reporting requirements addressed in this advisory. Written policies should be updated to reflect the amendments to the revised child abuse reporting requirements outlined below.
ACTION REQUIRED: Review and understand the amendments to Virginia Code § 63.2-1509.In the new subsection F, a required reporter (identified in subsection A) must report suspected child abuse or neglect within 24 hours of having reason to suspect a reportable offense. Under the new subsection C, a reason for suspicion includes any suspected violation of §§ 18.2-370 through 18.2-370.6 or § 18.2-374.3 involving a child. The statute’s requirements are further summarized below.
1. “Who is required to report suspected child abuse or neglect in Virginia?”
Overview: A Broad Mandatory Reporting Framework
Virginia’s mandatory reporting statute, Va. Code § 63.2-1509, requires a wide range of professionals who, in their professional or official capacity, have reason to suspect a child is abused or neglected to report immediately to the local department of social services or to the Department’s toll-free child abuse and neglect hotline. The list of mandatory reporters is extensive and includes:
Any person licensed to practice medicine or any of the healing arts
Any hospital resident or intern, and any person employed in the nursing profession
Any person employed as a social worker or family-services specialist
Any mental health professional
Any professional staff person employed by a private or state-operated hospital, institution, or facility to which children have been placed for care and treatment or committed
Any person 18 years of age or older associated with or employed by any public or private organization responsible for the care, custody, or control of children
Emergency medical services providers certified by the Board of Health
Any person who engages in the practice of behavior analysis, as defined in § 54.1-2900
This is not an exhaustive list. For health care institutions, virtually all clinical and support staff with patient contact — including physicians, nurses, therapists, social workers, and EMS personnel — may be mandatory reporters under Virginia law.
2. “What triggers a reporting obligation?”
Standard: Reason to Suspect
A reporting obligation arises when a covered professional has “reason to suspect” a child is abused or neglected. The current statute defines this standard as extending to three clinical scenarios:
Substance-affected newborns: A health care provider finding within six weeks of birth that the child was born affected by substance abuse or experiencing withdrawal symptoms from in utero drug exposure.
Substance-related diagnoses: A diagnosis made within four years of birth that the child has an illness, disease, or condition attributable to maternal abuse of a controlled substance during pregnancy.
Fetal Alcohol Spectrum Disorders: A diagnosis made within four years of birth that the child has a fetal alcohol spectrum disorder attributable to in utero alcohol exposure.
When “reason to suspect” is based on one of these clinical findings, that fact must be included in the report. Critically, such reports do not constitute a per se finding of child abuse or neglect.
The amended statute has expanded the definition of a “reason to suspect that a child is an abused or neglected child” to include any suspected violation of the offenses defined in Va. Code §§ 18.2-370 through 18.2-370.6 or § 18.2-374.3 involving a child.[1]
3. “How quickly must a report be made?”
The 24-Hour Reporting Deadline
Reports must be made as soon as possible, and not later than 24 hours after the covered professional has reason to suspect a reportable offense. A report not made within 24 hours may create compliance risk if the delay cannot be shown to be reasonable under the circumstances. The initial report may be oral but must be reduced to writing by the child abuse coordinator of the local department on a form prescribed by the Board of Social Services.
For employees of hospitals or similar institutions, a covered employee may, in lieu of making a direct report, immediately notify the person in charge of the institution or a designated person in charge, who must then make the report “forthwith.” If this internal notification route is used, the person in charge must:
Notify the original reporter when the report is made to the local department or the hotline
Provide the name of the individual who received the report
Forward any resulting communications, including information about actions taken, to the original reporter
All mandatory reporters who maintain records on the child must cooperate with investigating agencies and make related records available, subject to applicable federal law (including FERPA). Health care providers’ provision of such records is not prohibited by Virginia’s privacy statute in Va. Code § 8.01-399.
4. “What are the penalties for failing to report — and what changed in 2026?”
New Rule: Significantly Strengthened Criminal Penalties
The 2026 amendments added new penalty provisions to Va. Code § 63.2-1509 specifically targeting hospitals and similar facilities. The penalty structure is now as follows:
General Failures to Report (Subsection D/E):
First failure to timely report: civil fine of not more than $500
Subsequent failures: civil fine of not less than $1,000
Knowing and intentional failure where the reportable offense involves rape, sodomy, aggravated sexual battery, or object sexual penetration: Class 1 misdemeanor
NEW — Potential Healthcare Institutional Criminal Liability (New Subsection F): New subsection F, arguably the most significant addition to the statute, imposes heightened criminal liability specifically where the alleged abuse or neglect occurred at a private or state-operated hospital, institution, or facility to which children have been committed or placed for care and treatment as follows:
Failure to report as soon as possible and not longer than 24 hours after having reason to suspect a reportable offense: Class 1 misdemeanor (punishable by up to 12 months in jail and/or a $2,500 fine)
Second or subsequent conviction under this subsection: Class 6 felony (punishable by 1–5 years in prison, or up to 12 months in jail and/or a $2,500 fine at the court’s discretion)
This is a material escalation from prior law. Hospitals and other covered facilities should treat any employee’s failure to file a timely report as a potential criminal matter warranting immediate review by legal counsel.
5. “Are there protections for good-faith reporters?”
Immunity for Good-Faith Reports
Virginia law provides broad immunity for mandatory reporters. Under Va. Code § 63.2-1509(D) — renumbered in the 2026 amendments but preserved— any person who:
makes a report or provides records or information pursuant to the statute, or
testifies in any judicial proceeding arising from such report, records, or information
shall be immune from any civil or criminal liability or administrative penalty or sanction on account of such report, records, information, or testimony, unless the person acted in bad faith or with malicious purpose.
This immunity should be communicated clearly to all mandatory reporters within an institution to encourage timely and complete reporting.
6. “Are there any exceptions to the reporting obligation?”
Limited Exception: Actual Knowledge of Prior Report
Under the statute, no person is required to make a report if the person has actual knowledge that the same matter has already been reported to the local department or the Department’s toll-free child abuse and neglect hotline.[2] This exception is narrow: constructive knowledge or a general belief that someone else “likely reported” is insufficient. Institutions should not rely on this exception unless they can confirm that a specific, prior report has actually been filed.
Hospital and Health System Action Items
Immediately review and update internal mandatory reporting policies to reflect the new institutional penalty provisions (new Subsection F) and 24-hour deadline.
Train all clinical and administrative staff on who is a mandatory reporter, what triggers a reporting obligation, and how to make and document a report.
Designate and confirm reporting contacts (persons in charge or their designees) and ensure those individuals understand their obligation to report forthwith and notify the original reporter.
Educate staff of the broad immunity protection for good-faith reports.
Review any policies that might delay or discourage reporting and revise as appropriate to reduce potential criminal exposure for reporting delays.
Consult legal counsel immediately if a reporting failure is discovered at your institution, given the new Class 1 misdemeanor and Class 6 felony exposure.
References
[1] Va. Code § 63.2-1509(C), as amended by 2026 Va. Acts ch. 845 (H.B. 1414). [2] Va. Code § 63.2-1509(G) (formerly subsection E), as amended by 2026 Va. Acts ch. 845.
For questions about this advisory, please contact the Hancock Daniel & Johnson, LLC team at (804) 967-9604 or visit hancockdaniel.com.
The information contained in this advisory is for general educational purposes only. It is presented with the understanding that neither the author nor Hancock, Daniel & Johnson LLC, is offering any legal or other professional services. Since the law in many areas is complex and can change rapidly, this information may not apply to a given factual situation and can become outdated. Individuals desiring legal advice should consult legal counsel for up-to-date and fact-specific advice. Under no circumstances will the author or Hancock, Daniel & Johnson LLC be liable for any direct, indirect, or consequential damages resulting from the use of this material.
https://www.msv.org/wp-content/uploads/2021/11/msv-logo_340x156.png00varmshttps://www.msv.org/wp-content/uploads/2021/11/msv-logo_340x156.pngvarms2026-06-01 15:43:362026-06-01 15:43:37Virginia’s Amended Reporting Requirements and Penalties: What Hospitals, Health Systems, and Health Care Providers Need to Know About the 2026 Amendments to Va. Code § 63.2-1509
The Virginia Cannabis Control Authority (CCA) is pleased to share additional accredited online training courses on medical cannabis now available for healthcare practitioners.
In response to continued interest from practitioners, the CCA has expanded its partnership with TheAnswerPage.com to offer more optional, self-paced courses that support informed, evidence-based patient care.
This course provides evidence-based guidance on cannabis use disorder and cannabinoid hyperemesis syndrome. It covers clinical presentation, diagnostic criteria, screening tools, cannabis withdrawal, treatment strategies, and management of recurrent nausea and vomiting. Key concepts are reinforced through clinically relevant case scenarios.
This course offers a clear, evidence-based foundation to help clinicians counsel patients on cannabis use, evaluate therapeutic applications, and recognize potential risks. Topics include how cannabinoids work in the body, cannabinoid pharmacology, clinical effects, risks and contraindications, and cannabis-related disorders.
These new courses are in addition to the Virginia Medical Cannabis Program course bundle. All courses offer CME/CE credits and are designed for physicians, nurses, nurse practitioners, pharmacists, and dentists.
These trainings may be useful for all practitioners, not only those who issue medical cannabis certifications, as more patients are using cannabis products and seeking guidance from their providers.
Practitioners who choose to enroll can use the code VACANNABIS20 for 20% off at checkout.
You can learn more and register through the CCA website.
https://www.msv.org/wp-content/uploads/2021/11/msv-logo_340x156.png00varmshttps://www.msv.org/wp-content/uploads/2021/11/msv-logo_340x156.pngvarms2026-05-14 18:47:262026-05-14 19:03:01Additional Accredited Cannabis Training Now Available for Virginia Practitioners
The Virginia Department of Health (VDH) is announcing a measles outbreak in Buckingham County. As of May 13, VDH has identified twelve (12) outbreak-associated measles cases in the area. No patients reported recent travel. Without travel, the timing of these cases suggests local transmission. There are likely more measles cases than have been reported. In response, VDH is sharing important reminders and encouraging vaccination.
Vaccination Recommendations
The MMR vaccine is the best protection against measles. Please encourage your patients to be up to date with the routinely recommended number of MMR vaccinations.
Additionally, in the context of this outbreak, VDH encourages healthcare providers to talk to theirpatients who live in or visit the Buckingham County area about the following outbreakvaccination recommendations:
Infants aged 6 to 11 months are advised to get an early dose of the MMR vaccine. Infants who receive an early dose of MMR vaccine before their first birthday should receive two more doses at the recommended ages at least 28 days apart.
Children aged 12 months to 18 years old who have not yet been vaccinated or never hadmeasles infection should receive their first MMR vaccine dose with a second dose at least 28 days after the first dose.
Children aged 12 months or older who have previously received only one MMR dose should receive a second MMR vaccine dose at least 28 days after the first dose.
Adults born after 1957 who have not previously been vaccinated or never had measles infection should receive at least one dose of MMR vaccine. Adults in the following groups should receive two doses of MMR at least 28 days apart:
Attend school beyond high school (e.g. college, trade school).
Work or volunteer in a healthcare facility of any type.
Travel internationally, including on cruise ships.
Family or close contact of people with compromised immune systems.
People with HIV infection without severe immunosuppression.A small number (<5%) of adults vaccinated between 1963 1967 received an inactivated (killed) measles vaccine. Adults who received this type of vaccine, or do not know what type of vaccine they received between 1963–1967, should receive 1 or 2 doses of MMR vaccine.
Free or low-cost vaccines are available through Virginia’s Vaccines for Children (VFC) and Vaccines for Adults (VFA) programs for those who are eligible. If needed, you can locate a VFC or VFA provider on the VDH Website.
Measles Testing and Reporting
All Virginia healthcare providers should consult the updated VDH’s Measles Reporting and Testing Algorithm for suspected measles cases. Consider measles in patients with a fever and generalizedmaculopapular rash who:
were potentially exposed to a person with measles-like illness; OR
reside in Buckingham County or surrounding areas; OR
who have recently traveled out of the country or to regions of the United States reporting measles outbreaks.
Providers practicing in and around Buckingham County should maintain a high index ofsuspicion for measles and test any patient presenting with measles-compatible symptoms. This outbreak is also a good reminder to check the immune status of the healthcare providers on your teams.
If you suspect measles:
Isolate: Immediately isolate the patient in a single-patient airborne infection isolation room (AIIR), or in a private room with a closed door until an AIIR is available.
Test: Submit a nasopharyngeal (NP) swab in viral transport media or universal transport media for PCR testing and a serum specimen for testing at the Division of Consolidated Laboratory Services (DCLS). Follow instructions for specimen collection and handling. Test results are available in less than 24 hours.
Identify: Begin identifying staff, patients, and visitors who might have been exposed to the patient. If measles is confirmed, exposed people will need to be contacted and assessed for immunity.
Thank you for your continued partnership in keeping Virginians safe and healthy.
Sincerely,
B. Cameron Webb, MD, JD
State Health Commissioner
https://www.msv.org/wp-content/uploads/2021/11/msv-logo_340x156.png00varmshttps://www.msv.org/wp-content/uploads/2021/11/msv-logo_340x156.pngvarms2026-05-14 18:26:592026-05-14 18:27:03Measles Outbreak in Buckingham County
The Medicare Access and CHIP Reauthorization Act (MACRA) of 2015 consolidated three historic quality reporting programs into MIPS. MIPS requires physicians to report on quality measures, health IT measures, and improvement activities, creating significant administrative burden. The Centers for Medicare & Medicaid Services (CMS) also calculates cost measures and a new population health category (not-statutorily required) using claims data. CMS combines all of this data and generates a score of 0-100 points. Based on how their score compares to the national benchmark, physicians will see a penalty, a neutral payment adjustment, or a bonus. MIPS adjusts Medicare physician payment for all physicians unless they’re new to Medicare, qualifying alternative payment model participants, or have a low volume of Medicare patients or payments. The program is budget neutral. Penalties of up to -9 percent fund the bonuses.
Why are reforms to MIPS necessary?
MIPS disproportionately penalizes small and rural practices. Nearly 50 percent of solo eligible clinicians (ECs), 29 percent of small practices, and 18 percent of rural practices received a MIPS penalty in 2025 compared to fewer than 14 percent of ECs overall. Nearly 30 percent of solo ECs and 13 percent of small practices received the maximum -9 percent penalty compared to 2 percent of ECs overall.
MIPS is burdensome and costly. MIPS compliance costs $12,800 and requires 202 hours per physician per year according to a 2021 Journal of the American Medical Association(JAMA) Health Forum study.
MIPS does not measure quality and exacerbates health inequities. According to a 2022 JAMA study, MIPS scores are approximately as effective as chance in terms of identifying high versus low quality performance. Researchers found physicians providing high quality care but with low MIPS scores tended to have practices catering to a greater number of sicker and lower-income patients.
There are too few clinically relevant measures for specialists. MIPS scoring rules also disincentivize reporting on certain quality measures that are tailored to specialty care.
Introducing DPPS
It has been more than 10 years since MACRA passed, and change is urgently needed to reduce the harmful effects of MIPS. Designed as an alternative to MIPS, DPPS has been endorsed by the AMA, every state medical society, and more than 100 national specialty societies. DPPS would reset Medicare’s approach to improving quality and reducing avoidable costs by supporting small, rural and safety net practices; and increasing the clinical relevance of quality and cost measures to physicians and patients.
How does DPPS support small, rural, and safety net practices by reducing steep penalties?
DPPS would eliminate the win-lose tournament model and reduce the maximum penalty from -9 percent to one-half of a physician’s annual payment update (for example, 0.25 percent under current law or the increase in the Medicare Economic Index if H.R. 2474 passes), which is similar to other Medicare programs such as the Hospital Inpatient Quality Reporting Program.
It would reinvest penalties in quality improvement and alternative payment model readiness by assisting under-resourced practices with their value-based care transformation.
DPPS would freeze the performance threshold at 75 points for at least three years.
How does DPPS improve the clinical relevance and accuracy of cost and quality measures for physicians
and patients?
DPPS would incentivize CMS to fulfill its statutory obligations to share data on a quarterly basis, enabling physicians to improve performance on quality and cost measures.
Specifically, physicians who receive fewer than three MIPS performance feedback reports during the performance period would be exempt from any MIPS penalties.
With quarterly reports about which cost measures are being attributed to them, which patients are being assigned to them, and what costs outside of their practice they are being held accountable for, physicians can leverage this data to implement changes that would improve patient care and use resources more efficiently, saving money for the Medicare program, taxpayers, and beneficiaries.
Under the Data-driven Performance Payment System (DPPS):
Maximum penalties would be reduced from -9 percent of Medicare Physician Fee Schedule covered professional services to one-half of a physician’s annual update (e.g., 0.25 percent under current law or the increase in the Medicare Economic Index minus 1 percentage point as recommended by the Medicare Payment Advisory Commission), which is similar to other Medicare programs such as the Hospital Inpatient Quality Reporting Program.
Any penalties remaining after paying out bonuses would be reinvested penalties in quality improvement and alternative payment model readiness by assisting under-resourced practices with their value-based care transformation.
The 2023 Merit-based Incentive Payment System (MIPS) Performance Period included 541,421 total eligible clinicians (ECs). Here’s how 2023 MIPS scores would translate to Medicare payment adjustments under DPPS:
2.26 percent (12,236) of MIPS ECs received the maximum penalty of nine percent for not participating despite being eligible for MIPS in 2023. Under DPPS, this group would earn half of their payment update.
12.13 percent (65,674) scored below the 2023 performance threshold of 75 points and received a negative MIPS payment adjustment. Under DPPS, this group would receive three quarters of their payment update.
4.75 percent (25,717) scored 75 points and earned a neutral MIPS update. Under DPPS, they would earn their full update.
80.86 percent (437,793) scored above 75 points and earned a MIPS bonus. Under DPPS, they would receive up to 1.25 times their update. The remainder would be distributed to the improvement fund.
II. Mitigating Disproportionate Penalties on Certain Types of Practices to Stabilize Patient Access
2023 MIPS data shows that 29 percent of small practices, nearly 50 percent of solo practitioners, and 18 percent of rural practices received a MIPS penalty. With maximum MIPS penalties of 9 percent, this could significantly jeopardize access to care for vulnerable patient communities. Here is a breakdown of how DPPS payment adjustments would look for these practices based on 2023 MIPS data:
As shown below, DPPS would also level the playing field among specialties, thereby preserving access to primary and specialty care services particularly in rural and underserved areas.
DPPS would reinvest any remainingfunds collected through penalties not paid out in bonuses for high performers to small, rural, safety net, and other types of under-resourced practices to assist with value-based care transformation efforts. Funds could be used to hire care managers, purchase Certified Electronic Health Record Technology (CEHRT), and so on.
Moving Physicians to Value-Based Care:Merit-based Incentive Payment System (MIPS) Legislative Improvements
By replacing the current tournament model of payment adjustments with a more sustainable approach tied to annual payment updates and incentivizing CMS to share data with physicians, this legislation would stop the harmful penalties on small and rural practices while equipping physicians with timely feedback to improve care and reduce avoidable costs. This legislation would also rename the program as the Medicare Physician Data-Driven Performance Payment System (DPPS). DPPS would address two major shortcomings in MIPS:
1.Address Steep Penalties that Hurt Small and Rural Practices
Problem: MIPS subjects physicians to penalties of up to nine percent unless they meet onerous program requirements. Yet it is extremely burdensome and costly to participate and do well in MIPS. Compliance with MIPS costs $12,800 per physician per year and physicians spend 53 hours per year on MIPS-related tasks. This is why small, rural, and independent practices, along with practices that care for more patients who are dually eligible for Medicare and Medicaid, are more likely to be penalized, whereas large group practices, integrated systems, and alternative payment model participants are more likely to receive bonuses. The 2023 Quality Payment Program Experience Report shows that 29% of small practices, nearly 50% of solo practitioners, and 18% of rural practices received a MIPS penalty, which could jeopardize access to care for patients.
DPPS solutions:
Freeze the performance threshold at 75 to promote stability in MIPS. GAO will conduct a study in consultation with national medical specialty societies and make recommendations to Congress and HHS about an alternative threshold methodology.
Eliminate the MIPS win-lose style payment adjustments and instead link physicians’ MIPS performance to a portion of their annual payment update (e.g., 0.25% under MACRA or the percentage increase in MEI).
Reinvest penalties in bonuses for high performers, as well as investments in quality improvement and APM readiness with a targeted emphasis on assisting small, under-resourced practices.
2. Prioritize Timely and Actionable Data to Reduce Avoidable Costs and Improve Patient Outcomes
Problem: CMS has not met its statutory obligation1 to provide timely (e.g., quarterly) MIPS feedback reports and Medicare claims data to physicians. Instead, CMS issues a single feedback report after the performance period, up to 18 months after applicable services and care were provided.
DPPS solution: Hold CMS accountable for fulfilling its statutory obligations by exempting from DPPS penalties any physicians who do not receive at least three quarterly data reports during the performance period. These reports allow physicians to monitor their ongoing performance and identify gaps or variations in care that can be used to improve quality of care, care outcomes, and reduce costs.
1 §42 USC 1395w-4(q)(12) requires the Secretary to provide timely (e.g., quarterly) MIPS quality and cost feedback, as well as claims data feedback about items and services furnished to patients by other providers and suppliers, similar to data provided to Medicare Shared Savings Program accountable care organizations.
https://www.msv.org/wp-content/uploads/2021/11/msv-logo_340x156.png00varmshttps://www.msv.org/wp-content/uploads/2021/11/msv-logo_340x156.pngvarms2026-05-04 16:40:242026-05-04 16:40:24Data-Driven Performance Payment System (DPPS): Solving the Problems with the Merit-based Incentive Payment System (MIPS)