Data-Driven Performance Payment System (DPPS): Solving the Problems with the Merit-based Incentive Payment System (MIPS)
MIPS Background
The Medicare Access and CHIP Reauthorization Act (MACRA) of 2015 consolidated three historic quality reporting programs into MIPS. MIPS requires physicians to report on quality measures, health IT measures, and improvement activities, creating significant administrative burden. The Centers for Medicare & Medicaid Services (CMS) also calculates cost measures and a new population health category (not-statutorily required) using claims data. CMS combines all of this data and generates a score of 0-100 points. Based on how their score compares to the national benchmark, physicians will see a penalty, a neutral payment adjustment, or a bonus. MIPS adjusts Medicare physician payment for all physicians unless they’re new to Medicare, qualifying alternative payment model participants, or have a low volume of Medicare patients or payments. The program is budget neutral. Penalties of up to -9 percent fund the bonuses.
Why are reforms to MIPS necessary?
- MIPS disproportionately penalizes small and rural practices. Nearly 50 percent of solo eligible clinicians (ECs), 29 percent of small practices, and 18 percent of rural practices received a MIPS penalty in 2025 compared to fewer than 14 percent of ECs overall. Nearly 30 percent of solo ECs and 13 percent of small practices received the maximum -9 percent penalty compared to 2 percent of ECs overall.
- MIPS is burdensome and costly. MIPS compliance costs $12,800 and requires 202 hours per physician per year according to a 2021 Journal of the American Medical Association(JAMA) Health Forum study.
- MIPS does not measure quality and exacerbates health inequities. According to a 2022 JAMA study, MIPS scores are approximately as effective as chance in terms of identifying high versus low quality performance. Researchers found physicians providing high quality care but with low MIPS scores tended to have practices catering to a greater number of sicker and lower-income patients.
- There are too few clinically relevant measures for specialists. MIPS scoring rules also disincentivize reporting on certain quality measures that are tailored to specialty care.
Introducing DPPS
It has been more than 10 years since MACRA passed, and change is urgently needed to reduce the harmful effects of MIPS. Designed as an alternative to MIPS, DPPS has been endorsed by the AMA, every state medical society, and more than 100 national specialty societies. DPPS would reset Medicare’s approach to improving quality and reducing avoidable costs by supporting small, rural and safety net practices; and increasing the clinical relevance of quality and cost measures to physicians and patients.
How does DPPS support small, rural, and safety net practices by reducing steep penalties?
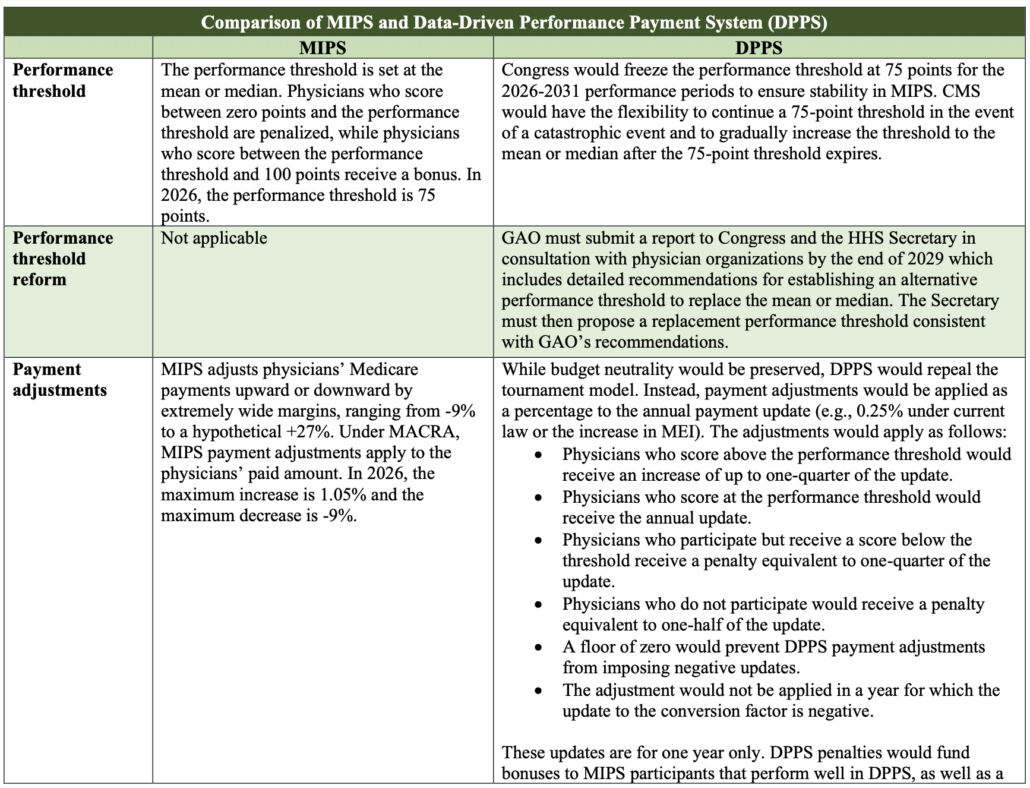
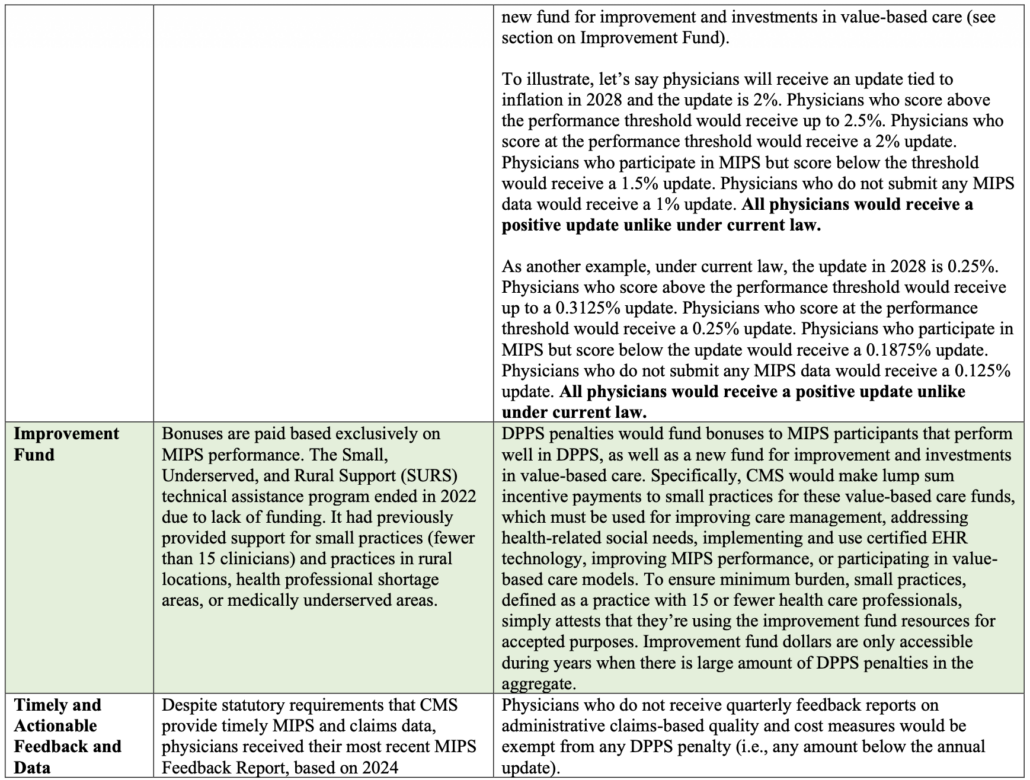
- DPPS would eliminate the win-lose tournament model and reduce the maximum penalty from -9 percent to one-half of a physician’s annual payment update (for example, 0.25 percent under current law or the increase in the Medicare Economic Index if H.R. 2474 passes), which is similar to other Medicare programs such as the Hospital Inpatient Quality Reporting Program.
- It would reinvest penalties in quality improvement and alternative payment model readiness by assisting under-resourced practices with their value-based care transformation.
- DPPS would freeze the performance threshold at 75 points for at least three years.
How does DPPS improve the clinical relevance and accuracy of cost and quality measures for physicians
and patients?
- DPPS would incentivize CMS to fulfill its statutory obligations to share data on a quarterly basis, enabling physicians to improve performance on quality and cost measures.
- Specifically, physicians who receive fewer than three MIPS performance feedback reports during the performance period would be exempt from any MIPS penalties.
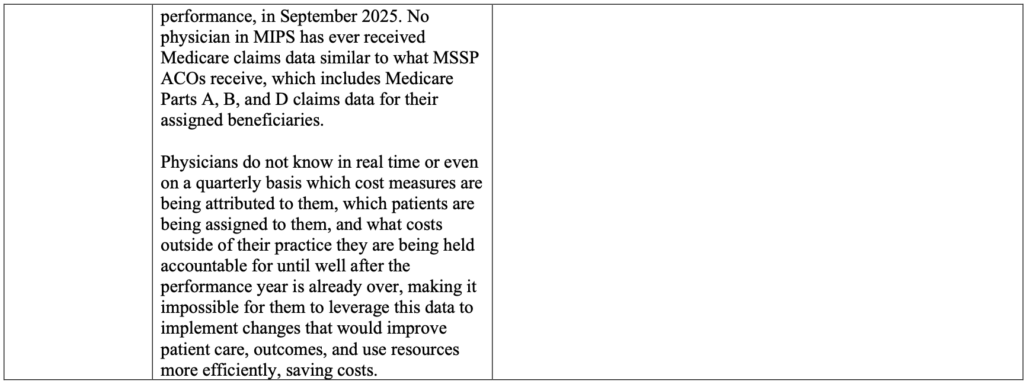
- With quarterly reports about which cost measures are being attributed to them, which patients are being assigned to them, and what costs outside of their practice they are being held accountable for, physicians can leverage this data to implement changes that would improve patient care and use resources more efficiently, saving money for the Medicare program, taxpayers, and beneficiaries.
DPPS would lower MIPS penalties and level the playing field
With insights from the 2023 MIPS Experience Data Report
I. Stabilizing Medicare Physician Payments
Under the Data-driven Performance Payment System (DPPS):
- Maximum penalties would be reduced from -9 percent of Medicare Physician Fee Schedule covered professional services to one-half of a physician’s annual update (e.g., 0.25 percent under current law or the increase in the Medicare Economic Index minus 1 percentage point as recommended by the Medicare Payment Advisory Commission), which is similar to other Medicare programs such as the Hospital Inpatient Quality Reporting Program.
- Any penalties remaining after paying out bonuses would be reinvested penalties in quality improvement and alternative payment model readiness by assisting under-resourced practices with their value-based care transformation.
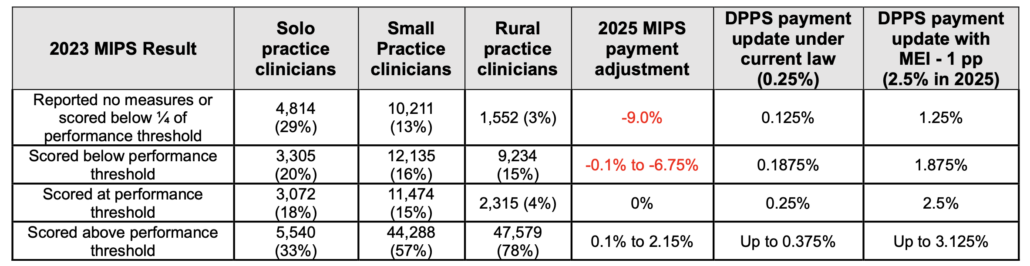
The 2023 Merit-based Incentive Payment System (MIPS) Performance Period included 541,421 total eligible clinicians (ECs). Here’s how 2023 MIPS scores would translate to Medicare payment adjustments under DPPS:
- 2.26 percent (12,236) of MIPS ECs received the maximum penalty of nine percent for not participating despite being eligible for MIPS in 2023. Under DPPS, this group would earn half of their payment update.
- 12.13 percent (65,674) scored below the 2023 performance threshold of 75 points and received a negative MIPS payment adjustment. Under DPPS, this group would receive three quarters of their payment update.
- 4.75 percent (25,717) scored 75 points and earned a neutral MIPS update. Under DPPS, they would earn their full update.
- 80.86 percent (437,793) scored above 75 points and earned a MIPS bonus. Under DPPS, they would receive up to 1.25 times their update. The remainder would be distributed to the improvement fund.
II. Mitigating Disproportionate Penalties on Certain Types of Practices to Stabilize Patient Access
2023 MIPS data shows that 29 percent of small practices, nearly 50 percent of solo practitioners, and 18 percent of rural practices received a MIPS penalty. With maximum MIPS penalties of 9 percent, this could significantly jeopardize access to care for vulnerable patient communities. Here is a breakdown of how DPPS payment adjustments would look for these practices based on 2023 MIPS data:
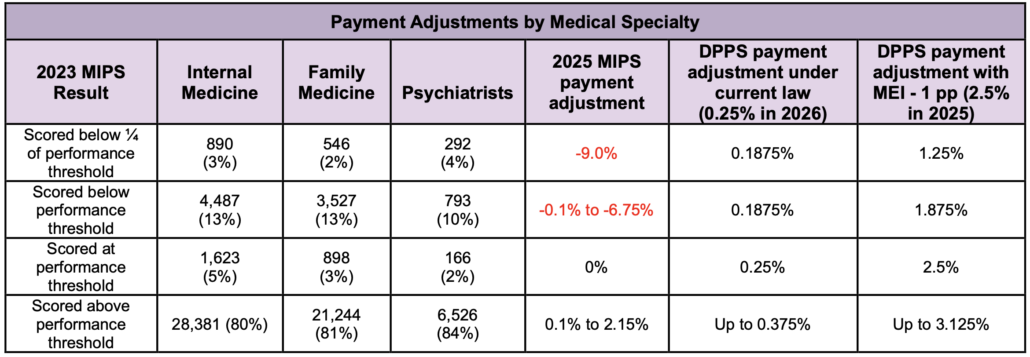
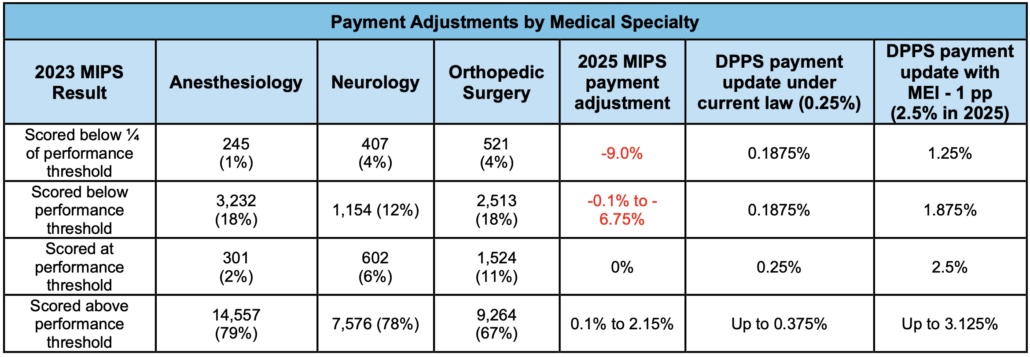
As shown below, DPPS would also level the playing field among specialties, thereby preserving access to primary and specialty care services particularly in rural and underserved areas.
DPPS would reinvest any remainingfunds collected through penalties not paid out in bonuses for high performers to small, rural, safety net, and other types of under-resourced practices to assist with value-based care transformation efforts. Funds could be used to hire care managers, purchase Certified Electronic Health Record Technology (CEHRT), and so on.
Moving Physicians to Value-Based Care: Merit-based Incentive Payment System (MIPS) Legislative Improvements
By replacing the current tournament model of payment adjustments with a more sustainable approach tied to annual payment updates and incentivizing CMS to share data with physicians, this legislation would stop the harmful penalties on small and rural practices while equipping physicians with timely feedback to improve care and reduce avoidable costs. This legislation would also rename the program as the Medicare Physician Data-Driven Performance Payment System (DPPS). DPPS would address two major shortcomings in MIPS:
1.Address Steep Penalties that Hurt Small and Rural Practices
Problem: MIPS subjects physicians to penalties of up to nine percent unless they meet onerous program requirements. Yet it is extremely burdensome and costly to participate and do well in MIPS. Compliance with MIPS costs $12,800 per physician per year and physicians spend 53 hours per year on MIPS-related tasks. This is why small, rural, and independent practices, along with practices that care for more patients who are dually eligible for Medicare and Medicaid, are more likely to be penalized, whereas large group practices, integrated systems, and alternative payment model participants are more likely to receive bonuses. The 2023 Quality Payment Program Experience Report shows that 29% of small practices, nearly 50% of solo practitioners, and 18% of rural practices received a MIPS penalty, which could jeopardize access to care for patients.
DPPS solutions:
- Freeze the performance threshold at 75 to promote stability in MIPS. GAO will conduct a study in consultation with national medical specialty societies and make recommendations to Congress and HHS about an alternative threshold methodology.
- Eliminate the MIPS win-lose style payment adjustments and instead link physicians’ MIPS performance to a portion of their annual payment update (e.g., 0.25% under MACRA or the percentage increase in MEI).
- Reinvest penalties in bonuses for high performers, as well as investments in quality improvement and APM readiness with a targeted emphasis on assisting small, under-resourced practices.
2. Prioritize Timely and Actionable Data to Reduce Avoidable Costs and Improve Patient Outcomes
Problem: CMS has not met its statutory obligation1 to provide timely (e.g., quarterly) MIPS feedback reports and Medicare claims data to physicians. Instead, CMS issues a single feedback report after the performance period, up to 18 months after applicable services and care were provided.
DPPS solution: Hold CMS accountable for fulfilling its statutory obligations by exempting from DPPS penalties any physicians who do not receive at least three quarterly data reports during the performance period. These reports allow physicians to monitor their ongoing performance and identify gaps or variations in care that can be used to improve quality of care, care outcomes, and reduce costs.
1 §42 USC 1395w-4(q)(12) requires the Secretary to provide timely (e.g., quarterly) MIPS quality and cost feedback, as well as claims data feedback about items and services furnished to patients by other providers and suppliers, similar to data provided to Medicare Shared Savings Program accountable care organizations.
Read discussion draft here.
